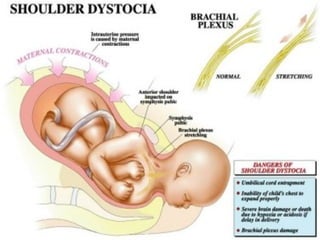
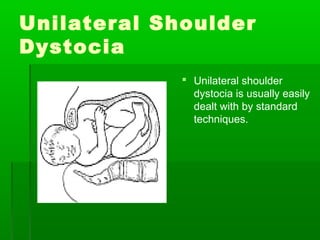
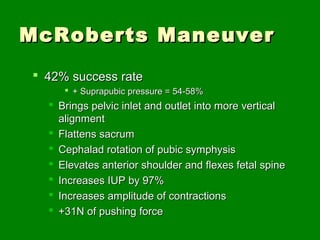
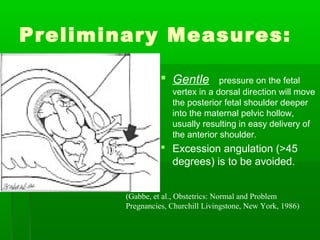
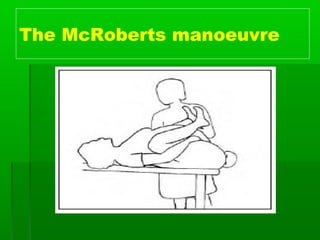
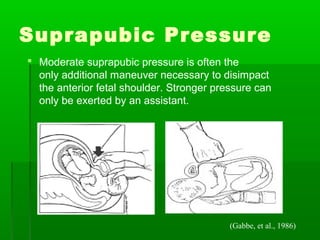
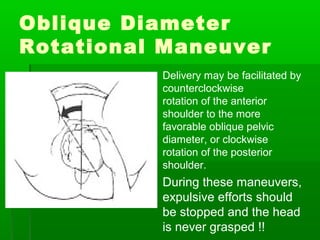
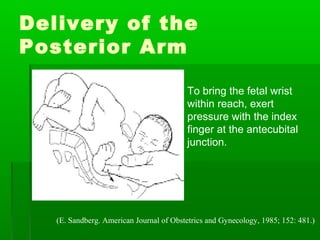
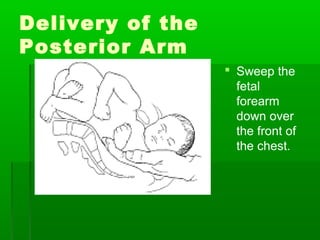
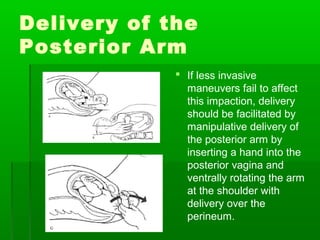
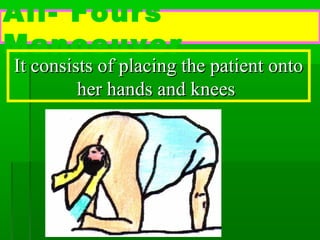
Shoulder dystocia occurs when the fetal shoulders become lodged at the maternal pelvis during birth, prolonging delivery. It represents an obstetric emergency. Risk factors include macrosomia, gestational diabetes, and prolonged labor. Management involves maneuvers like McRoberts position, suprapubic pressure, and rotational maneuvers to disimpact the shoulders. Complications for the baby include brachial plexus injury. Early diagnosis and treatment are important to prevent neonatal asphyxia. Simulation training is useful for practicing the management of shoulder dystocia.






























































![7-Shoulder_dystocia[1].pptx5555555555555555555555](https://cdn.slidesharecdn.com/ss_thumbnails/7-shoulderdystocia1-240901140722-b7a2771f-thumbnail.jpg?width=640&height=640&fit=bounds)





























