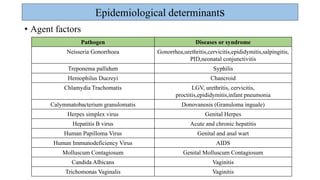
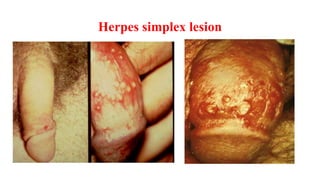
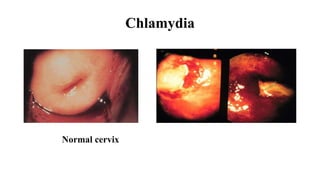
1. Sexually transmitted diseases (STDs) are caused by bacteria, viruses, parasites or fungi transmitted through sexual contact. Common STDs include chlamydia, gonorrhea, HIV/AIDS, herpes and syphilis.
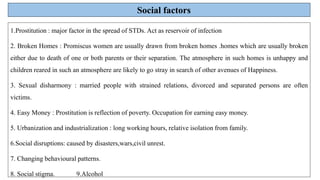
2. India has a major problem with STDs, with millions of new infections acquired each year. High-risk groups include sex workers, their clients like truck drivers, and individuals with multiple partners or broken homes.
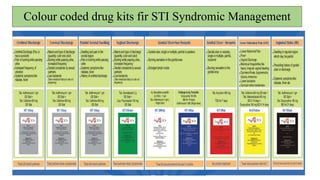
3. Syndromic management is used to clinically diagnose and treat STDs based on symptoms rather than definitive diagnostic testing. It is effective against mixed infections but can promote antibiotic resistance.