Download to read offline
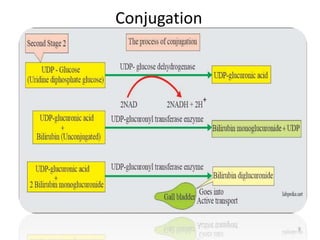
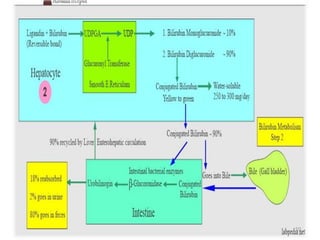
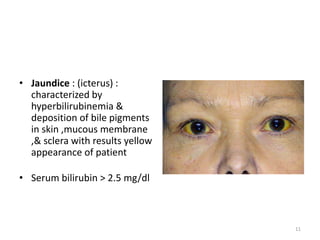
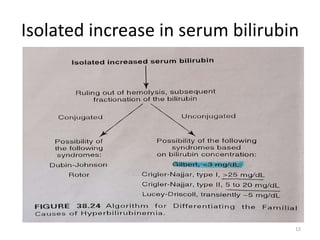
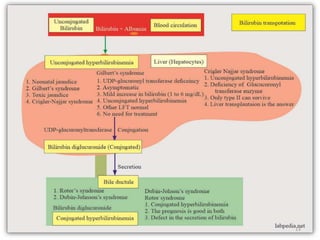
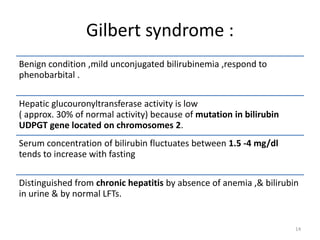
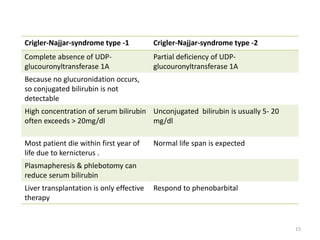
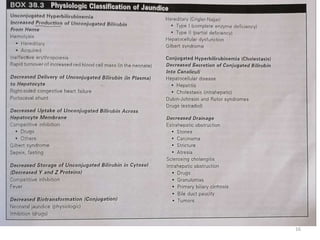

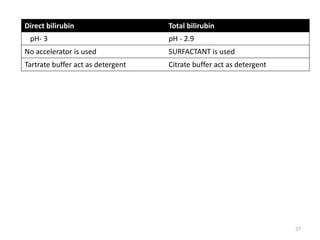

This document summarizes serum bilirubin, including its biochemistry, clinical significance, and analytical methods. Bilirubin is produced from the breakdown of hemoglobin in red blood cells. It exists in unconjugated and conjugated forms. The liver conjugates bilirubin so it can be excreted in bile and urine. Inherited disorders like Gilbert's syndrome and Crigler-Najjar syndrome affect bilirubin metabolism. Analytical methods to measure bilirubin include the diazo method and enzymatic methods. Total and direct bilirubin are measured to evaluate jaundice and liver function.







































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)













