Downloaded 107 times

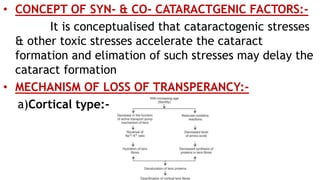
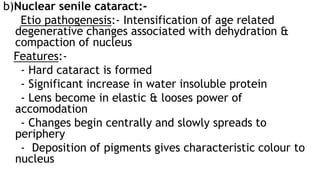
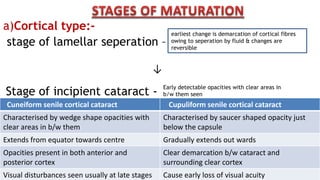
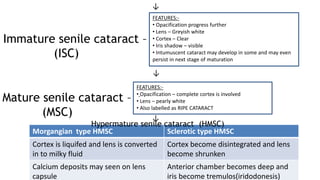
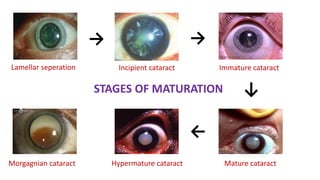
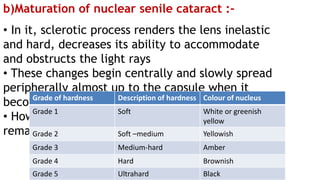
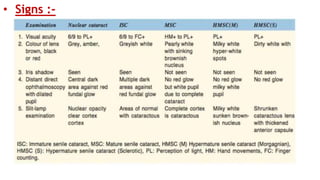
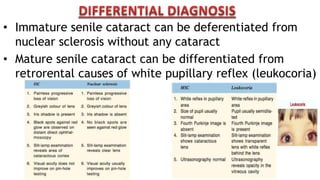


Opacification of the lens, known as cataract, is mainly caused by degeneration of normal lens fibers and is commonly seen in people over 50 years of age. There are two main types of cataracts: cortical/soft cataracts and nuclear/hard cataracts, which can co-exist in the same eye. Cataracts progress through stages from incipient to mature as opacity increases and spreads within the lens. Risk factors for earlier development of cataracts include age, heredity, UV exposure, nutritional deficiencies, smoking, and medical conditions like diabetes. Symptoms include glare, blurred or misty vision, and progressive loss of vision as opacity worsens.



































































