This document summarizes strategies for improving outcomes in ICU patients receiving sedation, including:
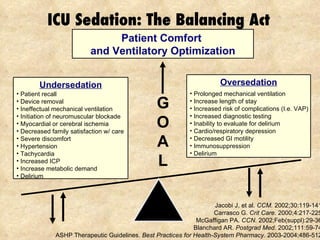
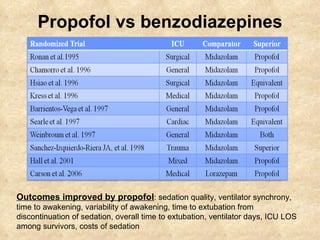
1) Using analgesia-first sedation and targeting light sedation to minimize risks of oversedation like longer duration of mechanical ventilation.
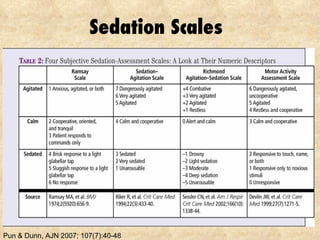
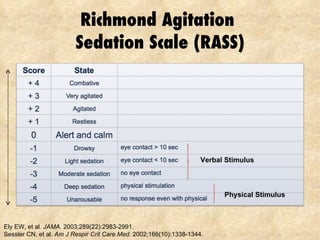
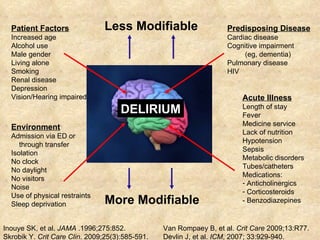
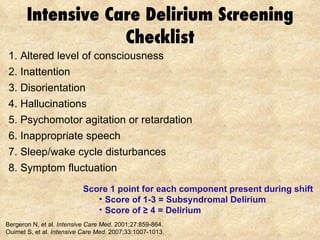
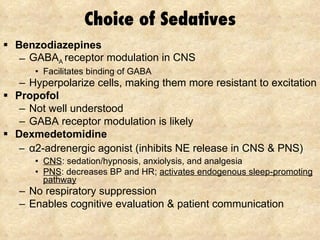
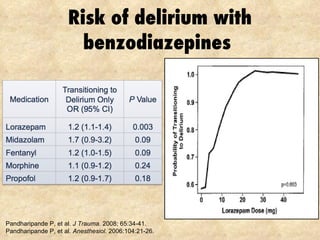
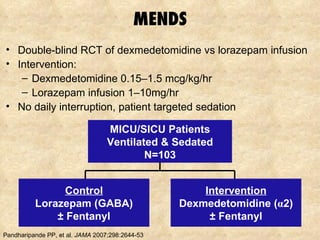
2) Regularly assessing sedation levels and pain to guide treatment. Non-benzodiazepine sedatives like dexmedetomidine may reduce risks of delirium.
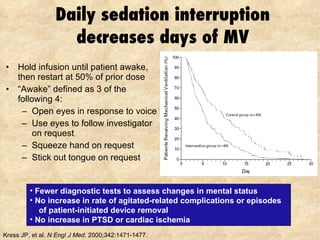
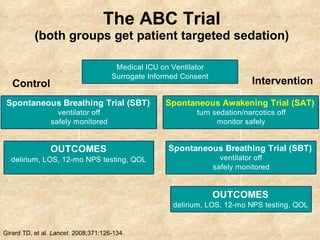
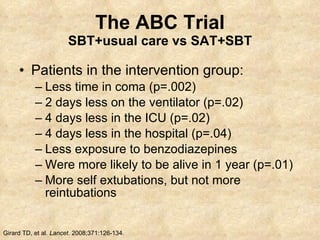
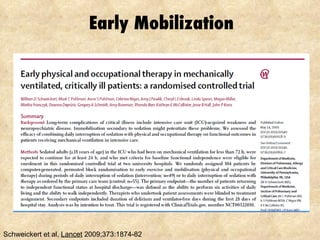
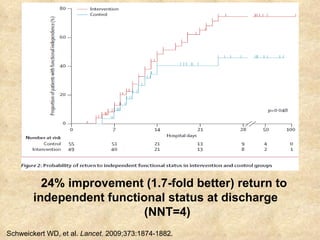
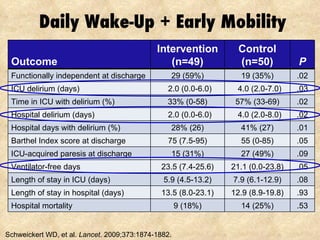
3) Daily sedation interruption or awakening trials combined with early mobility can decrease duration of mechanical ventilation and length of stay.


![Educational Delirium Website www.ICUdelirium.org [email_address] [email_address]](https://image.slidesharecdn.com/bogotasedation052110-100724183319-phpapp01/85/Bogota-sedation052110-53-320.jpg)








![Treatment Chronic Pain [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/treatmentchronicpainautosaved-220328083354-thumbnail.jpg?width=640&height=640&fit=bounds)





























































