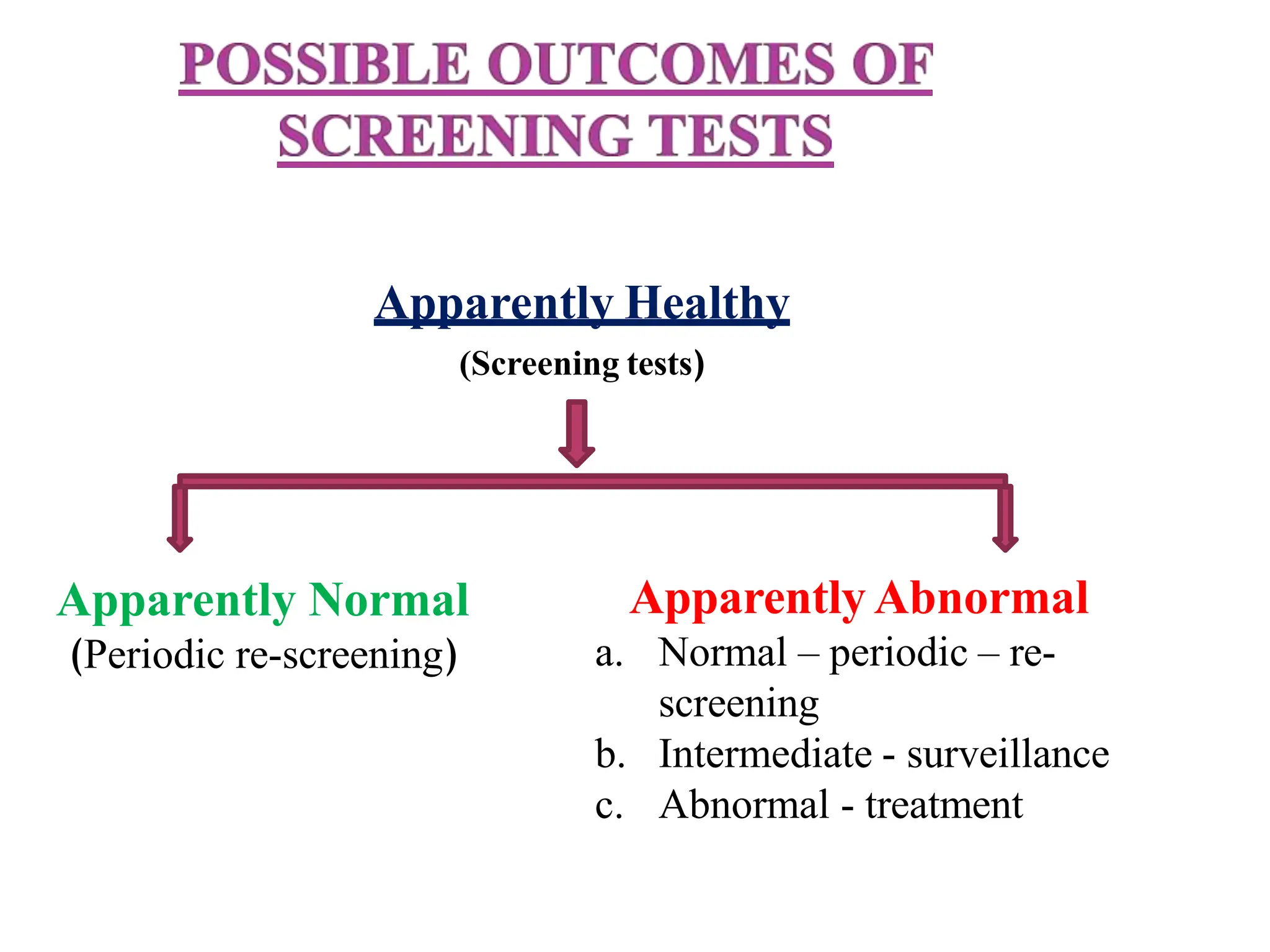
This document discusses screening, case finding, and diagnostic tests. Screening involves testing apparently healthy individuals to detect unrecognized disease early. Case finding uses clinical tests to detect disease in individuals seeking care for other reasons. Diagnostic tests are used to confirm or rule out disease in symptomatic patients. The document outlines criteria for screening such as having an important health problem detectable in early stages. It also discusses evaluating screening tests based on their acceptability, accuracy, yield, and simplicity. Factors influencing screening programs like disease prevalence and test characteristics are examined.