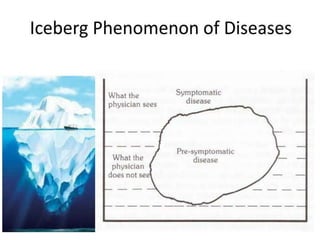
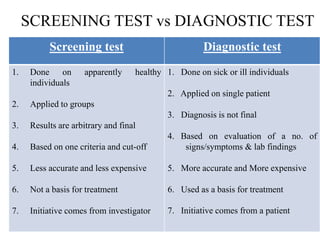
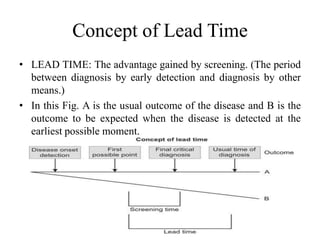
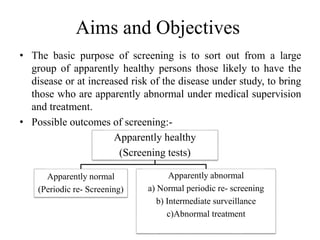
The document discusses screening for diseases. It defines screening as actively searching for unrecognized disease among apparently healthy people using tests or examinations. The goals of screening are to detect disease early when treatment can be most effective and to sort people into those who need medical follow up and those who do not. Key aspects discussed include the difference between screening and diagnostic tests, criteria for effective screening such as diseases amenable to screening, accurate and reliable screening tests, and evaluating screening programs.