Downloaded 187 times



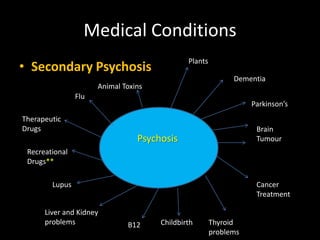
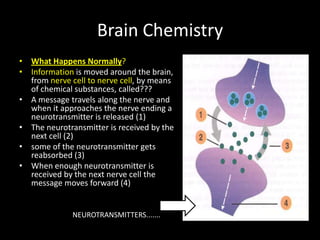

This document provides an overview of psychosis, including what it is, common symptoms, potential causes, and treatment options. It defines psychosis as a change in mental state involving hallucinations and delusions. Main symptoms are identified as hallucinations, delusions, thought disturbances, and lack of insight. Potential causes discussed include physical, substance-induced, medication-related, inherited vulnerability, traumatic experiences, and imbalances in neurotransmitters like dopamine and serotonin. First episode psychosis and first aid approaches are also summarized.

















































































