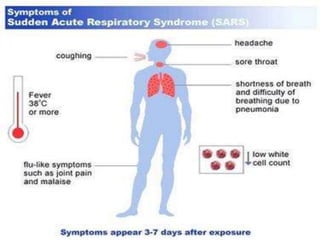
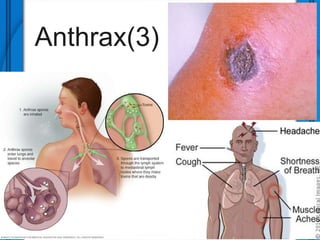
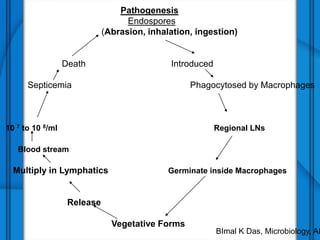
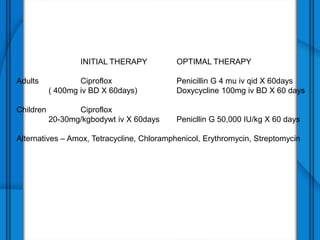
The document discusses Severe Acute Respiratory Syndrome (SARS) and Anthrax, including their causes, symptoms, transmission, diagnosis, and treatment options. SARS is caused by the SARS-CoV virus, while Anthrax is caused by Bacillus anthracis, with three clinical forms: cutaneous, pulmonary, and intestinal anthrax. Prevention measures for both diseases are emphasized, with no vaccine available for SARS and specific vaccination protocols for individuals at risk of Anthrax.