Downloaded 52 times
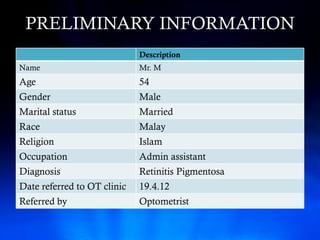
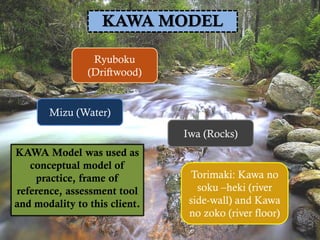
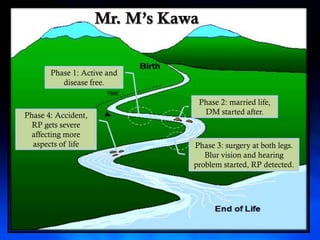
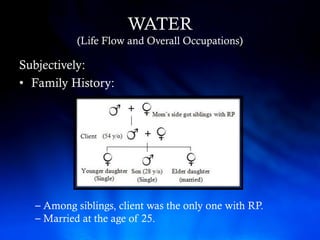
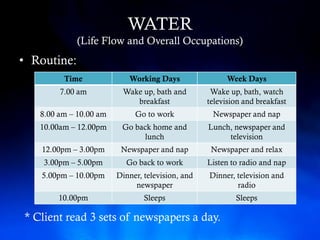
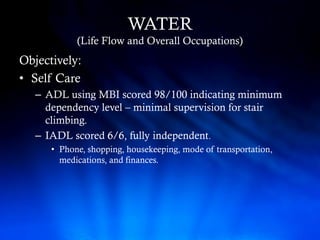
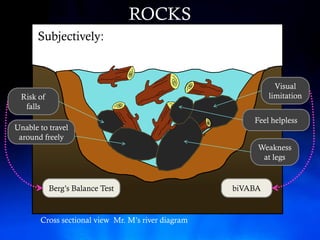
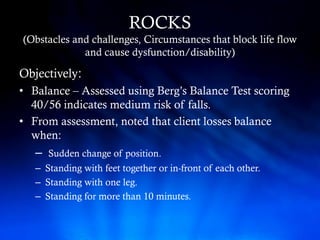
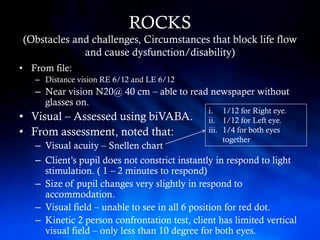
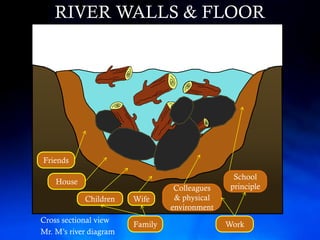
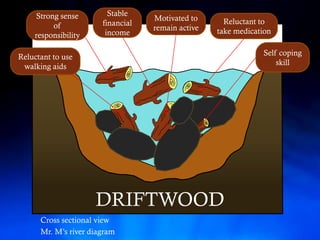
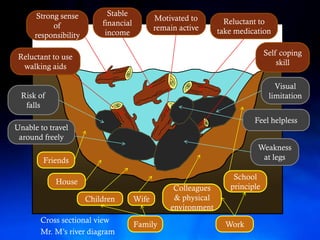
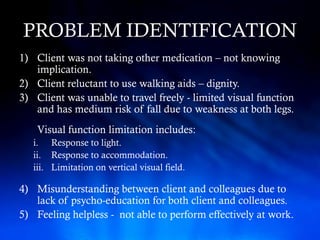
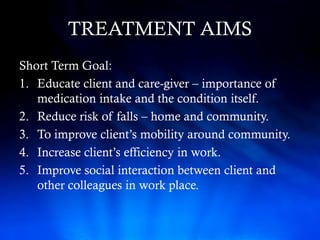
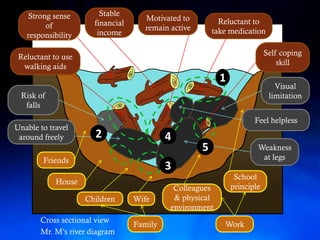
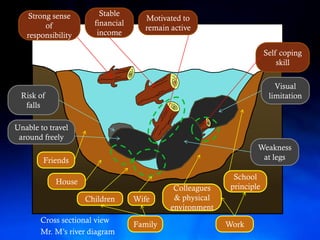

Mr. M is a 54-year-old man diagnosed with retinitis pigmentosa who was referred to occupational therapy for orientation and mobility training, and the Kawa model was used to assess his life flow, challenges, support system, and set goals to improve his independence, mobility, and work through education and environmental modifications.



































































