Download to read offline



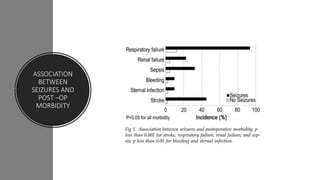

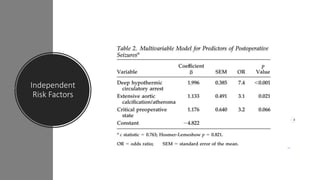


This study aimed to identify preoperative predictors of seizures after cardiac surgery and their impact on postoperative outcomes. The study analyzed 2578 patients who underwent cardiac procedures between 2007-2009. Seizures occurred in 1.2% of patients, usually within 2 days of surgery. Independent risk factors for seizures included critical preoperative states like ventricular fibrillation and the need for ionotropes or IABP. Patients who experienced seizures had higher rates of mortality, complications, and lower 1-year survival compared to those without seizures. The study found embolic infarcts on CT scans in 34% of seizure patients, suggesting cerebral embolism plays a role in postoperative seizures.







































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)















