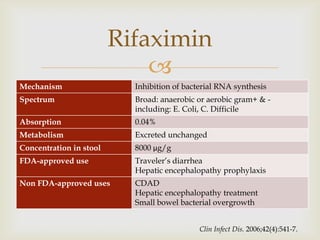
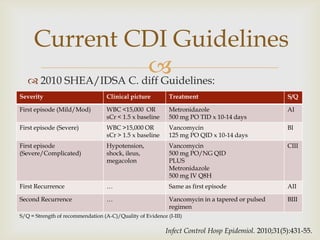
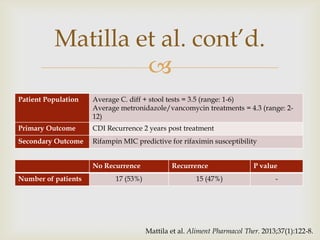
The document outlines a patient case of a 68-year-old male with recurrent Clostridium difficile infection (CDI) being considered for rifaximin treatment after standard therapy, as his symptoms persist post-vancomycin. It discusses the role of rifaximin in treating recurrent CDI, noting its mechanism and existing guidelines, while summarizing various studies that indicate its potential effectiveness and the need for further research. The overall conclusion suggests rifaximin may be beneficial for reducing recurrent diarrhea, although larger studies are required to confirm its safety and efficacy.









































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)











