Download to read offline
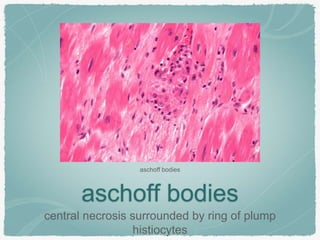
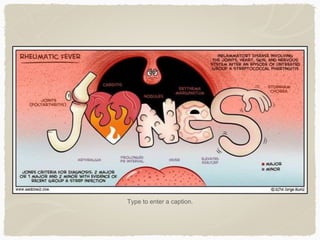
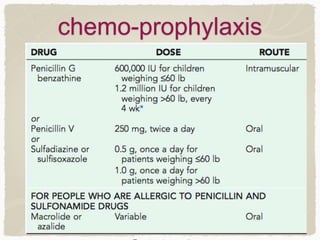
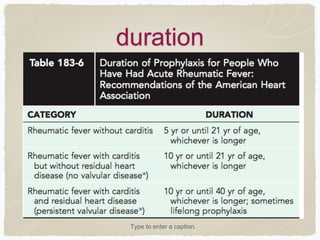

Rheumatic fever is an autoimmune disease that can develop after a streptococcal throat infection. It causes inflammation in connective tissues, especially the heart, joints, blood vessels, and skin. The inflammation is thought to be due to an immune cross-reaction between antigens in the streptococcal bacteria and human tissues. Symptoms vary depending on which tissues are affected but can include heart valve damage, arthritis, neurological disorders like chorea. Treatment involves antibiotics, salicylates like aspirin, and steroids depending on symptoms. Long term prevention requires ongoing antibiotics to prevent future streptococcal infections from triggering recurrences of rheumatic fever.