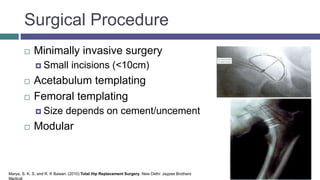
The retinacular arteries play an important role in vascularizing the femoral head. Their role increases in adulthood when epiphyseal cartilage blocks other vessels. Fractures of the femoral neck can disrupt these arteries, putting the head at risk. Both hip implants and resurfacing can also impact the retinacular arteries. Surgeons must consider various design factors for implants as well as potential complications.
![Vasculature of the femur
1. Illio-femoral artery
2. Ligamentum teres
3. Obturator artery
4. Femoral artery
5. Profunda femoris- 4a. perforating arteries
6. Lateral circumflex femoral artery (LCFA) -
5a. Ascending, 5b. Transverse and
5c.Descending
7. From the ascending – ascending cervical
arteries
8. Subsynovial
9. Medial circumflex artery
Pixgood.com, (2015). Pix For > Medial Circumflex Femoral Artery. [online] Available from: http://pixgood.com/medial-circumflex-femoral-artery.html
[Accessed 19 Mar. 2015].](https://image.slidesharecdn.com/anatomypresentationfinal-150326140729-conversion-gate01/85/Retinacular-arteries-3-320.jpg)
![Retinacular arteries
ALPF Medical Research, (2015). Vascular Supply To The Femoral Head. Femoral head. [online] Available from: http//http://www.alpfmedical.info/femoral-head/vascular-supply-to-
the-femoral-head.html [Acessed 17 Mar 2015].](https://image.slidesharecdn.com/anatomypresentationfinal-150326140729-conversion-gate01/85/Retinacular-arteries-4-320.jpg)
![Change in role from childhood to
adulthood.
LFCA and artery of ligamentum teres
Posterosuperior lateral epiphyseal and posteroinferior retinacular
branch -4 years
Metaphyseal vessels < 3 years old, after 14-17years
14-17 years
physis blocks metaphyseal.
anastomoses between metaphyseal-epiphyseal vessels.
Woon, C. (2015). Proximal Femur Fractures - Pediatric - Pediatrics - Orthobullets.com. [online] Orthobullets.com. Available at:
http://www.orthobullets.com/pediatrics/4018/proximal-femur-fractures--pediatric [Accessed 14 Mar. 2015].](https://image.slidesharecdn.com/anatomypresentationfinal-150326140729-conversion-gate01/85/Retinacular-arteries-6-320.jpg)
![Change in role from childhood to
adulthood.
Arteries- intramedullary at neck.
Anastomose with obturator artery.
Epiphyseal cartilage prevents retinacular artery
vascularising the head.
Virtual Anatomy Lab: Study notes. (2015). 1st ed. [ebook] Ottawa, p.1. Available at:
http://www.med.uottawa.ca/research/edemonstrator/w1/en/EN-study-notes-week-1.pdf [Accessed 19 Mar. 2015].](https://image.slidesharecdn.com/anatomypresentationfinal-150326140729-conversion-gate01/85/Retinacular-arteries-7-320.jpg)

![Polismed.com. Index of /upfiles/other/artgen/134 [Internet]. 2015 [cited 22 March 2015]. Available from:
http://www.polismed.com/upfiles/other/artgen/134/](https://image.slidesharecdn.com/anatomypresentationfinal-150326140729-conversion-gate01/85/Retinacular-arteries-11-320.jpg)
![Hip resurfacing
Adolescence/minor necrosis
Bone preservation
Bone is sculpted to accept a cap/short stem
Replacement acetabulum needed
Increased amount of femoral neck fracture
Heterotopic ossification
Laskin RS, Su EP, Padgett DE. Hip Resurfacing: an Overview [online]. Available from: http://www.hss.edu/conditions_hip-resurfacing-overview.asp#.VQ_lrfmzKG4 [Accessed
14/03/15]](https://image.slidesharecdn.com/anatomypresentationfinal-150326140729-conversion-gate01/85/Retinacular-arteries-13-320.jpg)