This document provides images and descriptions of various foot fractures, including:
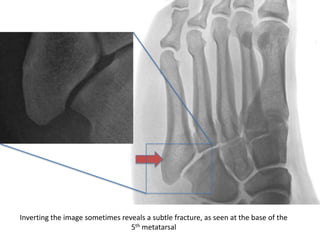
1) Phalangeal, calcaneal, cuboid, Jones, navicular, and LisFranc fractures. Subtle fractures can be easily missed on imaging.
2) Fracture treatment depends on displacement and stability, ranging from non-weight bearing casts to surgery for displaced or unstable fractures to reduce risk of nonunion.
3) Certain fractures like navicular have a high risk of avascular necrosis and may require open reduction and internal fixation.
4) Multiple fractures in a child should prompt consideration of non-accidental trauma.






















































































![Kin191 A. Ch.4. Foot. Toes. Inuries. Fall 2007[1]](https://cdn.slidesharecdn.com/ss_thumbnails/kin191a-ch-4-foot-toes-inuries-fall20071-090528145910-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)





























