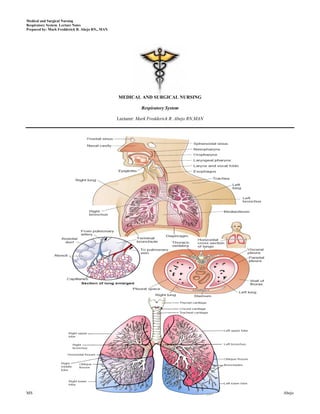
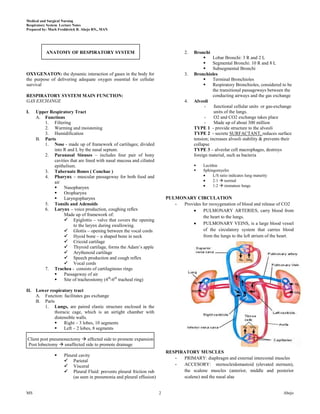







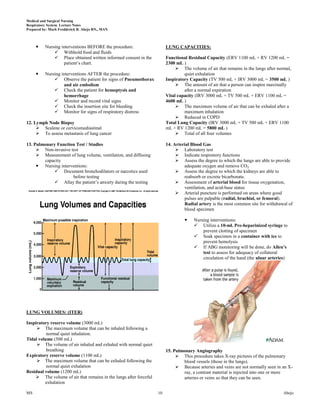










This document provides lecture notes on the respiratory system prepared by Mark Fredderick R. Abejo RN, MAN. It begins with the anatomy of the respiratory system including the upper respiratory tract, lower respiratory tract, lungs and pulmonary circulation. It then discusses the physiology of the respiratory system including ventilation, gas exchange, neurochemical control and the driving force for air flow. Finally, it outlines the respiratory examination and assessment including inspection of breathing patterns, cyanosis, the hands, face, trachea and chest as well as relevant medical history.