1. Lecture Notes on Cardiovascular System
Prepared By: Mark Fredderick R Abejo R.N, MAN
MEDICAL AND SURGICAL NURSING
Cardiovascular System
Lecturer: Mark Fredderick R. Abejo RN, MAN
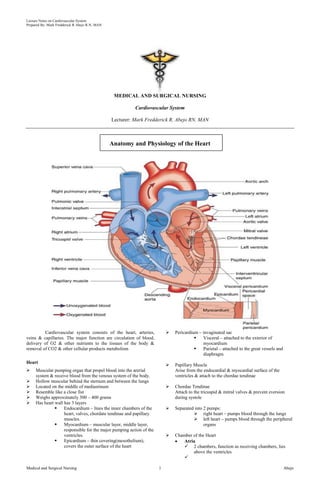
Anatomy and Physiology of the Heart
Cardiovascular system consists of the heart, arteries, Pericardium – invaginated sac
veins & capillaries. The major function are circulation of blood, Visceral – attached to the exterior of
delivery of O2 & other nutrients to the tissues of the body & myocardium
removal of CO2 & other cellular products metabolism Parietal – attached to the great vessels and
diaphragm
Heart
Papillary Muscle
Muscular pumping organ that propel blood into the arerial Arise from the endocardial & myocardial surface of the
system & receive blood from the venous system of the body. ventricles & attach to the chordae tendinae
Hollow muscular behind the sternum and between the lungs
Located on the middle of mediastinum Chordae Tendinae
Resemble like a close fist Attach to the tricuspid & mitral valves & prevent eversion
Weighs approximately 300 – 400 grams during systole
Has heart wall has 3 layers
Endocardium – lines the inner chambers of the Separated into 2 pumps:
heart, valves, chordate tendinae and papillary right heart – pumps blood through the lungs
muscles. left heart – pumps blood through the peripheral
Myocardium – muscular layer, middle layer, organs
responsible for the major pumping action of the
ventricles. Chamber of the Heart
Epicardium – thin covering(mesothelium), Atria
covers the outer surface of the heart 2 chambers, function as receiving chambers, lies
above the ventricles
Medical and Surgical Nursing 1 Abejo
2. Lecture Notes on Cardiovascular System
Prepared By: Mark Fredderick R Abejo R.N, MAN
Upper Chamber (connecting or receiving) Coronary Veins
Right Atrium: receives systemic venous blood Coronary sinus – main vein of the heart
through the superior vena cava, inferior vena cava & Great Cardiac vein – main tributary of the coronary sinus
coronary sinus Oblique vein – remnant of SVC, small unsignificant
Left Atrium: receives oxygenated blood returning to
the heart from the lungs trough the pulmonary veins
Heart Circulation
Ventricles
2 thick-walled chambers; major responsibility for
forcing blood out of the heart; lie below the atria
Lower Chamber (contracting or pumping)
Right Ventricle: contracts & propels deoxygenated
blood into pulmonary circulation via the aorta
during ventricular systole; Right atrium has
decreased pressure which is 60 – 80 mmHg
Left Ventricle: propels blood into the systemic
circulation via aortaduring ventricular systole; Left
ventricle has increased pressure which is 120 – 180
mmHg in order to propel blood to the systemic
circulation
Heart Valves
Tricuspid
Pulmonic
Mitral
Aortic
Cardiac Conduction System
Properties of Heart Conduction System
• Automaticity
• Excitability
Coronary artery – 1st branch of aorta • Conductivity
Right Coronary • Contractility
SA nodal Branch – supplies SA node
Right marginal Branch – supplies the right border
of the heart Structure of Heart Conduction System
AV nodal branch – supplies the AV node
Posterior interventricular artery – supplies both
ventricles
Left Coronary
Circumflex branch – supplies SA node in 40 % of
people
Left marginal – supplies the left ventricle
Anterior interventricular branch aka Left anterior
descending(LAD)–supplies both ventricles and
interventricular septum
Lateral branch – terminates in ant surface of the
heart
Nodal tissues
SA Node( Sino-atrial, Keith and Flack)
Primary Pacemaker
Between SVC and RA
Vagal and symphatetic innervation
Sinus Rhythms
Medical and Surgical Nursing 2 Abejo
3. Lecture Notes on Cardiovascular System
Prepared By: Mark Fredderick R Abejo R.N, MAN
AV Node( Atrioventricular , Kent and Tawara) The Normal Cardiac Cycle
At the right atrium
3 zones General Concepts
AN Zone(atrionodal) Systole - period of chamber contraction
N Zone (nodal) Diastole - period of chamber relaxation
NH zone (nodal –HIS) Cardiac cycle - all events of systole and diastole during one
heart flow cycle
Internodal and Interatrial Pathways
Connects SA and AV Node
Ant. Internodal(bachman) tract
Middle Internodal(wenkebach) tract Events of Cardiac Cycle
Posterior internodal(Thorel) tract 1. mid-to-late ventricular diastole: ventricles filled
Bundle of His/ Purkinje Fibers the AV valves are open
Provides for ventricular conduction system pressure: LOW in chambers; HIGH in
Fastest conduction among cardiac tissues aorta/pulmonary trunk
Right bundle aortic/pulmonary semilunar valves CLOSED
Left Bundle blood flows from vena cavas/pulmonary vein INTO
atria
Cardiac Action Potential blood flows through AV valves INTO ventricles
(70%)
Depolarization: electrical activation of a cell caused by
the influx of sodium into the cell while potassium exits 2. ventricular systole: blood ejected from heart
the cell filled ventricles begin to contract, AV valves
CLOSE
Repolarization: return of the cell to the resting state contraction of closed ventricles increases pressure
caused by re-entry of potassium into the cell while ventricular ejection phase - blood forced out
sodium exits semilunar valves open, blood -> aorta & pulmonary
trunk
Refractory periods:
Effective refractory period: phase in which cells 3. isovolumetric relaxation: early ventricular diastole
are incapable of depolarizing
Relative refractory period: phase in which cells ventricles relax, ventricular pressure becomes LOW
require a stronger-than-normal stimulus to semilunar valves close, aorta & pulmonary trunk
depolarize backflow
TOTAL CARDIAC CYCLE TIME = 0.8 second
Anatomical Sequence of Excitation of the Heart (normal 70 beats/minute)
(right atrium)
sinoatrial node (SA) atrial systole (contraction) = 0.1 second
(right AV valve) ventricular systole (contraction) = 0.3 second
atrioventricular node (AV) quiescent period (relaxation) = 0.4 second
atrioventricular bundle (bundle of His)
right & left bundle of His branches
Purkinje fibers of ventricular walls Cardiac Output - Blood Pumping of the Heart
(from SA through complete heart contraction = 220 ms = 0.22 s) General Concepts
• Stroke volume: the amount of blood ejected with each
a. Sinoatrial node (SA node) "the pacemaker" - has the heartbeat
fastest autorhythmic rate (70-80 per minute), and sets the • Cardiac output: amount of blood pumped by the
pace for the entire heart; this rhythm is called the sinus ventricle in liters per minute
rhythm; located in right atrial wall, just inferior to the • Preload: degree of stretch of the cardiac muscle fibers at
superior vena cava the end of diastole
• Contractility: ability of the cardiac muscle to shorten in
b. Atrioventricular node (AV node) - impulses pass from response to an electrical impulse
SA via gap junctions in about 40 ms.; impulses are • Afterload: the resistance to ejection of blood from the
delayed about 100 ms to allow completion of the ventricle
contraction of both atria; located just above tricuspid • Ejection fraction: the percent of end-diastolic volume
valve (between right atrium & ventricle) ejected with each heartbeat
c. Atrioventricular bundle (bundle of His) - in the
interATRIAL septum (connects L and R atria)
d. L and R bundle of His branches - within the
interVENTRICULAR septum (between L and R
ventricles)
e. Purkinje fibers - within the lateral walls of both the L and
R ventricles; since left ventricle much larger, Purkinjes
more elaborate here; Purkinje fibers innervate “papillary
muscles” before ventricle walls so AV can valves prevent
backflow
Medical and Surgical Nursing 3 Abejo
4. Lecture Notes on Cardiovascular System
Prepared By: Mark Fredderick R Abejo R.N, MAN
General Variables of Cardiac Output hypernatremia - HIGH Na+ concentration; can
block Na+ transport & muscle contraction
1. Cardiac Output (CO) - blood amount pumped per minute
CO (ml/min) = HR (beats/min) X SV (ml/beat) 3. Other Factors Effecting Heart Rate (HR)
Normal CO = 75 beats/min X 70 ml/beat
= 5.25 L/min normal heart rate - fetus 140 - 160 beats/minute
female 72 - 80 beats/minute
2. Heart Rate (HR) - cardiac cycles per minute male 64 - 72 beats/minute
Normal range is 60-100 beats per minute
Tachycardia is greater than 100 bpm 1. exercise - lowers resting heart rate (40-60)
Bradycardia is less than 60 bpm 2. heat - increases heart rate significantly
Sympathetic system INCREASES HR 3. cold - decreases heart rate significantly
Parasympathetic system (Vagus) DECREASES HR 4. tachycardia - HIGHER than normal resting heart rate
(over 100); may lead to fibrillation
3. Blood pressure - Cardiac output X peripheral resistance 5. bradycardia - LOWER than normal resting heart rate
Control is neural (central and peripheral) and (below 60); parasympathetic drug side effects; physical
hormonal conditioning; sign of pathology in non-healthy patient
Baroreceptors in the carotid and aorta
Hormones- ADH, aldosterone, epinephrine can
increase BP; ANF can decrease BP Vascular System
Regulation of Stroke Volume (SV) Major function of the blood vessels isto supply the tissue
End diastolic volume (EDV) - total blood collected in with blood, remove wastes, & carry unoxygenated blood
ventricle at end of diastole; determined by length of back to the heart
diastole and venous pressure (~ 120 ml)
End systolic volume (ESV) - blood left over in ventricle
at end of contraction (not pumped out); determined by Types of Blood Vessels
force of ventricle contraction and arterial blood pressure
(~50 ml)
Arteries
SV (ml/beat) = EDV (ml/beat) - ESV (ml/beat)
Normal SV = 120 ml/beat - 50 ml/beat = 70 ml/beat Elastic-walled vessels that can stretch during systole &
recoil during diastole; they carry blood away from the
Frank-Starling Law of the Heart - critical factor for stroke heart & distribute oxygenated blood throughout the body
volume is "degree of stretch of cardiac muscle cells"; Arterioles
more stretch = more contraction force
Small arteries that distribute blood to the capillaries &
increased EDV = more contraction force function in controlling systemic vascular resistance &
slow heart rate = more time to fill
exercise = more venous blood return therefore arterial pressure
Capilliaries
Regulation of Heart Rate (Autonomic, Chemical, Other) The following exchanges occurs in the capilliaries
O2 & CO2
1. Autonomic Regulation of Heart Rate (HR)
Solutes between the blood & tissue
Sympathetic - NOREPINEPHRINE (NE) increases heart Fluid volume transfer between the plasma &
rate (maintains stroke volume which leads to increased
Cardiac Output) interstitial space
Venules
Parasympathetic - ACETYLCHOLINE (ACh) decreases
heart rate Small veins that receive blood from capillaries &
function as collecting channels between the capillaries &
Vagal tone - parasympathetic inhibition of inherent rate
of SA node, allowing normal HR veins
Veins
Baroreceptors, pressoreceptors - monitor changes in
blood pressure and allow reflex activity with the Low-pressure vessels with thin small & less muscles than
autonomic nervous system
arteries; most contains valves that prevent retrograde
blood flow; they carry deoxygenated blood back to the
2. Hormonal and Chemical Regulation of Heart Rate (HR)
heart. When the skeletal surrounding veins contract, the
epinephrine - hormone released by adrenal medulla veins are compressed, promoting movement of blood
during stress; increases heart rate
back to the heart.
thyroxine - hormone released by thyroid; increases heart
rate in large quantities; amplifies effect of epinephrine
Ca++, K+, and Na+ levels very important;
hyperkalemia - increased K+ level; KCl used to
stop heart on lethal injection
hypokalemia - lower K+ levels; leads to
abnormal heart rate rhythms
hypocalcemia - depresses heart function
hypercalcemia - increases contraction phase
Medical and Surgical Nursing 4 Abejo
5. Lecture Notes on Cardiovascular System
Prepared By: Mark Fredderick R Abejo R.N, MAN
Palpation:
Assessment of the Client with Cardiovascular
Disorders
Nursing History
Risk Factors
A. Non – Modifiable Risk Factor
Age
Gender
Race
Heredity Heart Sounds: Stethoscope Listening
B. Modifiable Risk Factor Overview of Heart Sounds (lub-du ; lub, dub )
Stress
Diet lub - closure of AV valves, onset of ventricular systole
Exercise dub - closure of semilunar valves, onset of diastole
Sedentary lifestyle
Cigarette smoking Tricuspid valve (lub) - RT 5th intercostal, medial
Alcohol Mitral valve (lub) - LT 5th intercostal, lateral
Hypertension Aortic semilunar valve (dub) - RT 2nd intercostal
Hyperlipidemia Pulmonary semilunar valve (dub) - LT 2nd intercostals
DM
Obesity S1 - due to closure of the AV(mitral/tricuspid) valves
Type A personality - timing: beginning of systole
Contraceptive Pills - loudest at the apex
Common Clinical Manifestations of Cardiovascular Disorders S2 - due to the closure of the semi-lunar (pulmonic/aortic) valves
- timing: diastole
a. Dyspnea - loudest at the base
- Exertional
- Orthopnea
- Paroxysmal Noctural Dyspnea
- Cheyne-stokes
b. Chest Pain
c. Edema
- Ascites
- Hydrothorax
- Anasarca
d. Palpitation S3 – Ventricular Diastolic Gallop
e. Hemoptysis Mechanism: vibration resulting from resistance to rapid
f. Fatigue ventricular filling secondary to poor compliance
g. Syncope and Fainting Timing: early diastole
h. Cyanosis Location: Apex (LV) or LLSB (RV)
i. Abdominal Pain Pitch: faint and low pitched
j. Clubbing of fingers
k. Jaundice S4 - Atrial Diastolic Gallop
Mechanism: vibration resulting from resistance to late
Physical Assessment ventricular filling during atrial systole
Timing: late diastole ( before S1)
Inspection: Location: Apex ( LV) or LLSB (RV)
– Skin color Pitch: low ( use bell)
– Neck vein distention
Heart Murmurs
Murmur - sounds other than the typical "lub-dub"; typically caused
by disruptions in flow
Incompetent valve - swishing sound just AFTER the
normal "lub" or "dub"; valve does not completely close,
some regurgitation of blood
Stenotic valve - high pitched swishing sound when blood
should be flowing through valve; narrowing of outlet in
the open state
– Respirations
– Pulsations Pericardial Friction Rub
– Clubbing
– Capillary refill It is an extra heart sound originating from the pericardial sac
Mechanism: Originates from the pericardial sac as it moves
Timing: with each heartbeat
Medical and Surgical Nursing 5 Abejo
6. Lecture Notes on Cardiovascular System
Prepared By: Mark Fredderick R Abejo R.N, MAN
Location: over pericardium. Upright position, leaning 2. Coagulation Screening Test
forward
Pitch: high pitched and scratchy. Sounds like sandpaper a. Bleeding Time – measures the ability to stop bleeding after
being rubbed together small puncture wound
Significance: inflammation, infection, infiltration
b. Partial Thromboplastin Time (PTT) – used to identify
deficiencies of coagulation factors, prothrombin and fibrinogen;
Classification of Clients with Diseases of the monitors heparin therapy.
Heart ( Functional Capacity )
c. Prothrombin Time (Pro-time) – determines activity and
Class I. Patients with cardiac disease but without interaction of the Prothrombin group: factors V (preacclerin), VII
resulting limitations of physical activity. (proconvertin), X (Stuart-Power factor), prothrombin and
Class II. Patients with cardiac disease resulting to slight fibrinogen; used to determine dosages of oral anti-coagulant.
limitation of physical activity
Class III. Patients with cardiac disease resulting in Normal Values
marked limitation of physical activity. They are
comfortable at rest. Bleeding Time: 2.75-8 min
Class IV. Patients with cardiac disease resulting in Partial Thromboplastin Time (PTT): 60 - 70 sec.
inability to carry on any physical activity without Prothrombin Time (PT): 12-14 sec.
discomfort
Diagnostic Assessment 3. Erythrocyte sedimentation rate ( ESR)
It is a measurement of the rate at which RBC’s settle out
Purposes: of anticoagulated blood in an hour
It is elevated in infectious heart disorder or myocardial
1. To assist in diagnosing MI infarction
2. To identify abnormalities
3. To assess inflammation Normal Values
4. To determine baseline value Male: 15-20 mm/hr
5. To monitor serum level of medications Female: 20-30 mm/hr
6. To assess the effects of medications
4. CARDIAC Proteins and enzymes
A. Blood Studies
a. CK- MB ( creatine kinase)
1. Complete Blood Count Most cardiac specific enzymes
Accurate indicator of myocardial dammage
a. RBC count- # of RBCs/ mm3 of blood, to diagnose anemia and Elevates in MI within 4 hours, peaks in 18 hours and
ploycythemia then declines till 3 days
Normal value is 0-7 U/L or males 50-325 mu/ml
b. Hemoglobin- # of grams of hgb/ 100ml of blood; to measure the Female 50-250 mu/ml
oxygen-carrying capacity of the blood
b. Lactic Dehydrogenase (LDH)
c. Hematocrit – expressed in %; measures the volume of RBCs in Most sensitive indicator of myocardial damage
proportion to plasma; used also to diagnose anemia and Elevates in MI in 24 hours, peaks in 48-72 hours
polycythemia and abnormal hydration states Return to normal in 10-14 days
Normally LDH1 is greater than LDH2
d. RBC indices- measure RBC size and hemoglobin content Lactic Dehydrogenase (LDH)
a. MCV (mean corpuscular volume) MI- LDH2 greater than LDH1 (flipped LDH pattern)
b. MCH (mean corpuscular hemoglobin) Normal value is 70-200 IU/L (100 – 225 mu/ml)
c. MCHC (mean corpuscular hemoglobin concentrarion)
c. Myoglobin
e. Platelet count- # of Platelet/ mm3; to diagnose Rises within 1-3 hours
thrombocytopenia and subsequent bleeding tendencies Peaks in 4-12 hours
Returns to normal in a day
f. WBC count- of WBCs/ mm3 of blood; to detect infection or Not used alone
inflammation Muscular and RENAL disease can have elevated
myoglobin
g. WBC Differential count- determines proportion of each WBC
in a sample of 100 WBCs; used to classify leukemias d. Troponin I and T
Troponin I is usually utilized for MI
Normal Values Elevates within 3-4 hours, peaks in 4-24 hours and
persists for 7 days to 3 weeks!
RBC: Women – 4.2-5.4 million/mm3 Normal value for Troponin I is less than 0.6 ng/mL
Men – 4.7-6.1 million/mm3 REMEMBER to AVOID IM injections before
Hgb: Women – 12-16 g/dl obtaining blood sample!
Men – 13-18 g/dl Early and late diagnosis can be made!
Hct : Women – 36-42%
Men – 42-48% e. SERUM LIPIDS
WBC: 5000-10,000/mm3 Lipid profile measures the serum cholesterol,
Granulocytes triglycerides and lipoprotein levels
Neutrophils: 55-70% Cholesterol= 200 mg/dL
Eosinophils: 1-4% Triglycerides- 40- 150 mg/dL
Basophils: 0.5-1.0% LDH- 130 mg/dL
Agranulocytes HDL- 30-70- mg/dL
Lymphocytes: 20-40% NPO post midnight (usually 12 hours)
Monocytes: 2-8%
Platelets: 150,000-450,000/mm3
Medical and Surgical Nursing 6 Abejo
7. Lecture Notes on Cardiovascular System
Prepared By: Mark Fredderick R Abejo R.N, MAN
B. Non-Invasive Procedure
1. Cardiac Monitoring / Electrocardiography (ECG)
A non-invasive procedure that evaluates the electrical
activity of the heart
a. Limb Leads
b. Precordial Leads
Deflection Waves of ECG
1. P wave - initial wave, demonstrates the depolarization from SA
Node through both ATRIA; the ATRIA contract about 0.1 s after
start of P Wave.
2. QRS complex - next series of deflections, demonstrates the
depolarization of AV node through both ventricles; the ventricles
contract throughout the period of the QRS complex, with a short
delay after the end of atrial contraction; repolarization of atria also
obscured
The precordial leads VI –V6 are part of the 12 lead EKG. 3. T Wave - repolarization of the ventricles (0.16 s)
They are not monitored with the standard limb leads
4. PR (PQ) Interval - time period from beginning of atrial
contraction to beginning of ventricular contraction (0.16 s)
c. 12 lead ECG
5. QT Interval - the time of ventricular contraction (about 0.36 s);
from beginning of ventricular depolarization to end of
repolarization.
2. Holter Monitoring
A non-invasive test in which the client wears a Holter
monitor and an ECG tracing recorded continuously over
a period of 24 hours
Instruct the client to resume normal activities and
maintain a diary of activities and any symptoms that may
develop
ECG Paper
Medical and Surgical Nursing 7 Abejo
8. Lecture Notes on Cardiovascular System
Prepared By: Mark Fredderick R Abejo R.N, MAN
3. Stress Test
A non-invasive test that studies the heart during C. Invasive Procedure
activity and detects and evaluates CAD
Exercise test, pharmacologic test and emotional test 1. Cardiac Catheterization ( Coronary Angiography /
Treadmill testing is the most commonly used stress Arteriography )
test Insertion of a catheter into the heart and surrounding
Used to determine CAD, Chest pain causes, drug vessels
effects and dysrhythmias in exercise Is an invasive procedure during which physician
Pre-test: consent may be required, adequate rest , eat injects dye into coronary arteries and immediately
a light meal or fast for 4 hours and avoid smoking, takes a series of x-ray films to assess the structures
alcohol and caffeine of the arteries
During the test: secure electrodes to appropriate Determines the structure and performance of the
location on chest, obtain baseline BP and ECG heart valves and surrounding vessels
tracing, instruct client to exercise as instructed and Used to diagnose CAD, assess coronary atery
report any pain, weakness and SOB, monitor BP and patency and determine extent of atherosclerosis
ECG continuously, record at frequent interval Pretest: Ensure Consent, assess for allergy to
Post-test: instruct client to notify the physician if seafood and iodine, NPO, document weight and
any chest pain, dizziness or shortness of breath . height, baseline VS, blood tests and document the
Instruct client to avoid taking a hot shower for 10-12 peripheral pulses
hours after the test Pretest: Fasting for 8-12 hours, teachings,
medications to allay anxiety
Intra-test: inform patient of a fluttery feeling as the
4. Pharmacological stress test catheter passes through the heart; inform the patient
Use of dipyridamole that a feeling of warmth and metallic taste may
Maximally dilates coronary artery occur when dye is administered
Side-effect: flushing of face Post-test: Monitor VS and cardiac rhythm
Pre-test: 4 hours fasting, avoid alcohol, caffeine Monitor peripheral pulses, color and warmth and
Post test: report symptoms of chest pain sensation of the extremity distal to insertion site
Maintain sandbag to the insertion site if required to
maintain pressure
Monitor for bleeding and hematoma formation
5. ECHOCARDIOGRAM
Non-invasive test that studies the structural and
functional changes of the heart with the use of ultrasound
Client Preparation: instruct client to remain still during
the test, secure electrodes for simultaneous ECG tracing, 2. Nuclear Cardiology
explain that there will be no pain or electrical shock, Are safe methods of evaluating left ventricular muscle
lubricant placed on the skin will be cool. function and coronary artery blood distribution.
Client Preparation: obtain written consent, explain
procedure, instruct client that fasting may be required for
6. Phonocardiography a short period before the exam, assess for iodine allergy.
Is a graphic recording of heart sound with simultaneous Post Procedure: encourage client to drink fluids to
ECG. facilitate the excretion of contrast material, assess
venipuncture site for bleeding or hematoma.
Types of Nuclear Cardiology
o Multigated acquisition (MUGA) or cardiac
blood pool scan
Provides information on wall motion
during systole and diastole, cardiac
valves, and EF.
o Single-photon emission computed
tomography (SPECT)
Used to evaluate the myocardium at
risk of infarction and to determine
infarction size.
o Positron emission tomography (PET)
scanning
Uses two isotopes to distinguish
viable and nonviable myocardial
tissue.
Medical and Surgical Nursing 8 Abejo
9. Lecture Notes on Cardiovascular System
Prepared By: Mark Fredderick R Abejo R.N, MAN
o Perfusion imaging with exercise testing
Determines whether the coronary Client Preparation: obtain consent, insertion is under
blood flow changes with increased strict sterile technique, usually at the bedside, explain to
activity. client the sterile drapes may cover the face, assists to
Used to diagnose CAD, determine position client flat or slight T-postion as tolerated and
the prognosis in already diagnosed instruct to remain still during the procedure
CAD, assess the physiologic Nursing Care During Insertion: Monitor and document
significance of a known coronary HR,BP and ECG during the procedure
lesion, and assess the effectiveness of
various therapeutic modalities such
as coronary artery bypass surgery,
percutaneous coronary intervention, CARDIAC DISORDER
or thrombolytic therapy.
D. Hemodynamics Monitoring CORONARY ARTERIAL DISEASE
ISCHEMIC HEART DISEASE
1. CVP ( Central Venous Pressure )
Reflects the pressure of the blood in the right atrium.
Engorgement is estimated by the venous column that can Results from the focal narrowing of the large and
be observed as it rises from an imagined angle at th point medium-sized coronary arteries due to deposition of atheromatous
of manubrium ( angle of Louis). plaque in the vessel wall
With normal physiologic condition, the jugular venous
column rises no higher than 2-3 cm above the clavicle
Stages of Development of Coronary Artery Disease
with the client in a sitting position at 45 degree angle.
1. Myocardial Injury: Atherosclerosis
2. Myocardial Ischemia: Angina Pectoris
3. Myocardial Necrosis: Myocardial Infarction
CVP is a measurement of:
- cardiac efficiency I. ATHEROSCLEROSIS
- blood volume
- peripheral resistance ATHEROSCLEROSIS ARTERIOSCLEROSIS
Right ventricular pressure – a catheter is passed from a
cutdown in the antecubital, subclavian jugular or basilica Narrowing of artery Hardening of artery
vein to the right atrium and attached to a prescribed Lipid or fat deposits Calcium and protein
manometer or tranducer. deposits
Tunica intima
NORMAL CVP is 2 -8 cm h20 or 2-6 mm Hg Tunica media
Decrease indicates dec. circulating volume, increase
indicates inc. blood volume or right heart beat failure.
A. PRESDISPOSING FACTORS
To Measure: patient should be flat with zero point of
1. Sex: male
manometer at the same level of the RA which
2. Race: black
corresponds to the mid-axillary line of the patient or
3. Smoking
approx. 5 cm below the sternum.
4. Obesity
Fluctuations follow patients respiratory function and will
5. Hyperlipidemia
fall on inspiration and rise on expiration due to changes
6. Sedentary lifestyle
in intrapulmonary pressure. Reading should be obtained
7. Diabetes Mellitus
at the highest point of fluctuation.
8. Hypothyroidism
9. Diet: increased saturated fats
10. Type A personality
2. Pulmonary Artery Pressure ( PAP) Monitoring
Appropriate for critically ill clients requiring more
B. SIGNS AND SYMPTOMS
accurate assessments of the left heart pressure
1. Chest pain
Swan-Ganz Catheter / Pulmonary Artery Catheter is use
2. Dyspnea
3. Tachycardia
4. Palpitations
5. Diaphoresis
C. TREATMENT
Percutaneous Transluminal Coronary Angioplasty and
Intravascular Stenting
Mechanical dilation of the coronary vessel wall by
compresing the atheromatous plaque.
It is recommended for clients with single-vessel
coronary artery disease.
Medical and Surgical Nursing 9 Abejo
10. Lecture Notes on Cardiovascular System
Prepared By: Mark Fredderick R Abejo R.N, MAN
Prosthetic intravascular cylindric stent maintain Nursing Management:
good luminal geometry after ballon deflation and
withdrawal. Nitroglycerine is the drug of choice for relief of pain
Intravascular stenting is done to prevent restenosis from acute ischemic attacks
after PTCA Instruct to avoid over fatigue
Plan regular activity program
For Saphenous Vein Site:
Wear support stocking 4-6 week postop
Apply pressure dressing or sand bag on the site
Keep leg elevated when sitting
3 Complications of CABG
1. Pneumonia: encourage to perform deep breathing,
coughing exercise and use of incentive spirometer
2. Shock
3. Thrombophlebitis
II. ANGINA PECTORIS
Transient paroxysmal chest pain produced by insufficient
blood flow to the myocardium resulting to myocardial
ischemia
Clinical syndrome characterized by paroxysmal chest
pain that is usually relieved by rest or nitroglycerine due
to temporary myocardial ischemia
Types of Angina Pectoris
Stable Angina: pain less than 15 minutes, recurrence is less
frequent.
Unstable Angina : pain is more than 15 mins.,but not less
than 30 minutes, recurrence is more frequent and the
Coronary Arterial Bypass Graft Surgery
intensity of pain increases.
Variant Angina ( Prinzmetal’s Angina ): Chest pain is on
longer duration and may occur at rest. Result from coronary
vasospasm.
Angina Decubitus: paroxysmal chest pain that occur when
the client sits or stand.
A. PRESDISPOSING FACTORS
1. Sex: male
2. Race: black
3. Smoking
4. Obesity
5. Hyperlipidemia
6. Sedentary lifestyle
Greater and lesser saphenous veins are commonly used for 7. Diabetes Mellitus
bypass graft procedures 8. Hypertension
9. CAD: Atherosclerosis
10. Thromboangiitis Obliterans
11. Severe Anemia
12. Aortic Insufficiency: heart valve that fails to open &
close efficiently
13. Hypothyroidism
14. Diet: increased saturated fats
15. Type A personality
B. PRESIPITATING FACTORS
4 E’s of Angina Pectoris
1. Excessive physical exertion: heavy exercises, sexual
activity
2. Exposure to cold environment: vasoconstriction
3. Extreme emotional response: fear, anxiety,
excitement, strong emotions
4. Excessive intake of foods or heavy meal
C. SIGNS AND SYMPTOMS
1. Levine’s Sign: initial sign that shows the hand
clutching the chest
2. Chest pain: characterized by sharp stabbing pain
Objectives of CABG located at sub sterna usually radiates from neck,
1. Revascularize myocardium back, arms, shoulder and jaw muscles usually
2. To prevent angina relieved by rest or taking nitroglycerine(NTG)
3. Increase survival rate 3. Dyspnea
4. Done to single occluded vessels 4. Tachycardia
5. If there is 2 or more occluded blood vessels CABG is 5. Palpitations
done 6. Diaphoresis
Medical and Surgical Nursing 10 Abejo
11. Lecture Notes on Cardiovascular System
Prepared By: Mark Fredderick R Abejo R.N, MAN
Propanolol: not given to COPD cases: it causes
D. DIAGNOSTIC PROCEDURE bronchospasm and DM cases: it cause
1. History taking and physical exam hypoglycemia
2. ECG: may reveals ST segment depression & T wave Side Effects: Nausea and vomiting, mental
inversion during chest pain depression and fatigue
3. Stress test / treadmill test: reveal abnormal ECG
during exercise
4. Increase serum lipid levels C. Calcium – Channel Blockers: relaxes smooth
5. Serum cholesterol & uric acid is increased cardiac muscle, reduces coronary vasospasm
Amlodipine ( norvasc )
E. MEDICAL MANAGEMENT Nifedipine ( calcibloc )
1. Drug Therapy: if cholesterol is elevated Diltiazem ( cardizem )
Nitrates: Nitroglycerine (NTG) Assess HR and BP
Beta-adrenergic blocking agent: Propanolol Adminester 1 hour before meal and 2 hours
Calcium-blocking agent: nefedipine after meal ( foods delay absorption )
Ace Inhibitor: Enapril
2. Modification of diet & other risk factors 4. Administer oxygen inhalation
3. Surgery: Coronary artery bypass surgery 5. Place client on semi-to high fowlers position
4. Percutaneuos Transluminal Coronary Angioplasty 6. Monitor strictly V/S, I&O, status of
(PTCA) cardiopulmonary fuction & ECG tracing
7. Provide decrease saturated fats sodium and caffeine
F. NURSING INTERVENTIONS 8. Provide client health teachings and discharge
1. Enforce complete bed rest planning
2. Give prompt pain relievers with nitrates or narcotic Avoidance of 4 E’s
analgesic as ordered Prevent complication (myocardial infarction)
3. Administer medications as ordered: Instruct client to take medication before
indulging into physical exertion to achieve the
A. Nitroglycerine(NTG): when given in small maximum therapeutic effect of drug
doses will act as venodilator, but in large doses Reduce stress & anxiety: relaxation techniques
will act as vasodilator & guided imagery
Give 1st dose of NTG: sublingual 3-5 Avoid overexertion & smoking
minutes Avoid extremes of temperature
Give 2nd dose of NTG: if pain persist after Dress warmly in cold weather
giving 1st dose with interval of 3-5 Participate in regular exercise program
minutes Space exercise periods & allow for rest periods
Give 3rd& last dose of NTG: if pain still The importance of follow up care
persist at 3-5 minutes interval
9. Instruct the client to notify the physician
NTG Tablets(sublingual) immediately if pain occurs & persists despite rest &
Keep the drug in a dry place, avoid medication administration
moisture and exposure to sunlight as it
may inactivate the drug
Change stock every 6 months
Offer sips of water before giving
III. MYOCARDIAL INFARCTION
sublingual nitrates, dryness of mouth may
inhibit drug absoprtion
Relax for 15 minutes after taking a tablet: Death of myocardial cells from inadequate oxygenation,
to prevent dizziness often caused by sudden complete blockage of a coronary
Monitor side effects: orthostatic artery
hypotension, flushed face. Transient Characterized by localized formation of necrosis (tissue
headache & dizziness: frequent side effect destruction) with subsequent healing by scar formation &
Instruct the client to rise slowly from fibrosis
sitting position Heart attack
Assist or supervise in ambulation Terminal stage of coronary artery disease characterized
by malocclusion, necrosis & scarring.
NTG Nitrol or Transdermal patch Types of M.I
Nitropatch is applied once a day, usually Transmural Myocardial Infarction: most dangerous type
in the morning. characterized by occlusion of both right and left coronary
Avoid placing near hairy areas as it may artery
decrease drug absorption Subendocardial Myocardial Infarction: characterized by
Avoid rotating transdermal patches as it occlusion of either right or left coronary artery
may decrease drug absorption
Avoid placing near microwave ovens or The Most Critical Period Following Diagnosis of
during defibrillation as it may lead to Myocardial Infarction
burns (most important thing to remember) 6-8 hours because majority of death occurs due to
arrhythmia leading to premature ventricular contractions
B. Beta-blockers: decreases myocardial oxygen (PVC)
demand by decreasing heart rate, cardiac output
and BP A. PREDISPOSING FACTORS
Propanolol 1. Sex: male
Metropolol 2. Race: black
Pindolol 3. Smoking
Atenolol 4. Obesity
Assess PR, withhold if dec.PR 5. CAD: Atherosclerotic
Administer with food ( prevent GI upset ) 6. Thrombus Formation
7. Genetic Predisposition
8. Hyperlipidemia
Medical and Surgical Nursing 11 Abejo
12. Lecture Notes on Cardiovascular System
Prepared By: Mark Fredderick R Abejo R.N, MAN
9. Sedentary lifestyle 2. Administer oxygen low flow 2-3 L / min: to prevent
10. Diabetes Mellitus respiratory arrest or dyspnea & prevent arrhythmias
11. Hypothyroidism 3. Enforce CBR in semi-fowlers position without bathroom
12. Diet: increased saturated fats privileges(use bedside commode): to decrease cardiac
13. Type A personality workload
4. Instruct client to avoid forms of valsalva maneuver
B. SIGNS AND SYMPTOMS 5. Place client on semi fowlers position
1. Chest pain 6. Monitor strictly V/S, I&O, ECG tracing & hemodynamic
Excruciating visceral, viselike pain with sudden procedures
onset located at substernal& rarely in 7. Perform complete lung / cardiovascular assessment
precordial 8. Monitor urinary output & report output of less than 30 ml
Usually radiates from neck, back, shoulder, / hr: indicates decrease cardiac output
arms, jaw & abdominal muscles (abdominal 9. Provide a full liquid diet with gradual increase to soft diet:
ischemia): severe crushing low in saturated fats, Na & caffeine
Not usually relieved by rest or by 10. Maintain quiet environment
nitroglycerine 11. Administer stool softeners as ordered:to facilitate bowel
2. N/V evacuation & prevent straining
3. Dyspnea 12. Relieve anxiety associated with coronary care
4. Increase in blood pressure & pulse, with gradual unit(CCU)environment
drop in blood pressure (initial sign) 13. Administer medication as ordered:
5. Hyperthermia: elevated temp a. Vasodilators:Nitroglycirine (NTG), Isosorbide
6. Skin: cool, clammy, ashen Dinitrate, Isodil (ISD): sublingual
7. Mild restlessness & apprehension b. Anti Arrythmic Agents: Lidocaine (Xylocane),
8. Occasional findings: Brithylium
Pericardial friction rub Side Effects: confusion and dizziness
Split S1& S2 c. Beta-blockers: Propanolol (Inderal)
Rales or Crackles upon auscultation d. ACE Inhibitors: Captopril (Enalapril)
S4 or atrial gallop e. Calcium Antagonist: Nefedipine
f. Thrombolytics / Fibrinolytic Agents: Streptokinase,
C. DIAGNOSTIC PROCEDURED Urokinase, Tissue Plasminogen Activating Factor
1. Cardiac Enzymes (TIPAF)
CPK-MB: elevated Side Effects:allergic reaction, urticaria, pruritus
Creatinine phosphokinase(CPK):elevated Nursing Intervention: Monitor for bleeding
time
Heart only, 12 – 24 hours
g. Anti Coagulant
Lactic acid dehydrogenase(LDH): is increased
Heparin
Serum glutamic pyruvate transaminase(SGPT):
Antidote: Protamine Sulfate
is increased
Nursing Intervention: Check for Partial
Serum glutamic oxal-acetic
transaminase(SGOT): is increased Thrombin Time (PTT)
2. Troponin Test: is increased Caumadin(Warfarin)
3. ECG tracing reveals Antidote:Vitamin K
ST segment elevation Nursing Intervention: Check for
T wave inversion Prothrombin Time (PT)
Widening of QRS complexes: indicates that h. Anti Platelet: PASA (Aspirin): Anti thrombotic
effect
there is arrhythmia in MI
Side Effects:Tinnitus, Heartburn, Indigestion /
Dyspepsia
Contraindication:Dengue, Peptic Ulcer Disease,
Unknown cause of headache
14. Provide client health teaching & discharge planning
concerning:
a. Effects of MI healing process & treatment regimen
b. Medication regimen including time name purpose,
schedule, dosage, side effects
c. Dietary restrictions: low Na, low cholesterol,
avoidance of caffeine
d. Encourage client to take 20 – 30 cc/week of wine,
whisky and brandy:to induce vasodilation
e. Avoidance of modifiable risk factors
f. Prevent Complication
4. Serum Cholesterol & uric acid: are both increased
5. CBC: increased WBC Arrhythmia: caused by premature ventricular
contraction
D. NURSING INTERVENTIONS Cardiogenic shock: late sign is oliguria
Left Congestive Heart Failure
Goal: Decrease myocardial oxygen demand Thrombophlebitis: homan’s sign
Stroke / CVA
1. Decrease myocardial workload (rest heart) Dressler’s Syndrome(Post MI Syndrome):client
Establish a patent IV line is resistant to pharmacological agents:
Administer narcotic analgesic as ordered: Morphine administer 150,000-450,000 units of
Sulfate IV: provide pain relief(given IV because streptokinase as ordered
after an infarction there is poor peripheral perfusion g. Importance of participation in a progressive activity
& because serum enzyme would be affected by IM program
injection as ordered) h. Resumption of ADL particularly sexual intercourse:
Side Effects: Respiratory Depression is 4-6 weeks post cardiac rehab, post CABG &
Antidote: Naloxone (Narcan) instruct to:
Side Effects of Naloxone Toxicity: is tremors
Medical and Surgical Nursing 12 Abejo
13. Lecture Notes on Cardiovascular System
Prepared By: Mark Fredderick R Abejo R.N, MAN
Make sex as an appetizer rather than dessert Aminophylline to reduce
Instruct client to assume a non weight bearing bronchospasm caused by severe
position congestion.
Client can resume sexual intercourse: if can Vasodilators to reduce venous return
climb or use the staircase Diuretics to decrease circulating
i. Need to report the ff s/sx: volume
Increased persistent chest pain
Dyspnea V. PERICARDITIS / DRESSLER’S SYNDROME
Weakness
Fatigue Is the inflammation of the pericardium which occurs
Persistent palpitation approximately 1 – 6 weeks after AMI.
Light headedness Results as an antigen – antibody response. The necrotic
j. Enrollment of client in a cardiac rehabilitation tissues play the role of an antigen, which trigger antibody
program formation. Inflammatory process follows.
k. Strict compliance to mediation & importance of Constrictive Pericarditis is a condition in which a chronic
follow up care inflammatory thickening of the pericardium compresses
the heart so that it is unable to fill normally during
diastole.
IV. CARDIOGENIC SHOCK ( POWER/PUMP FAILURE )
A. SIGNS AND SYMPTOMS
Is a shock state which result from profound left 1. Pain in the anterior chest, aggravated by coughing,
ventricular failure usually from massive MI. yawning, swallowing, twisting and turning the torso,
It result to low cardiac output, thereby systemic relieved by upright, leaning forward position.
hypoperfusion. 2. Pericardial friction rub – scratchy, grating or
cracking sound
A. SIGNS AND SYMPTOMS 3. Dyspnea
1. Decrease systolic BP 4. Fever, sweating, chills
2. Oliguria 5. Joints pains
3. Cold, clammy skin 6. Arrhythmias
4. Weak pulse
5. Cyanosis B. NURSING INTERVENTIONS
6. Mental lethargy
7. Confusion 1. Elevate head of bed, place pillow on the overbed
table so that the patient can lean on it.
B. MEDICAL MANAGEMENT 2. Bed rest
1. Counterpulsation ( mechanical cardiac assistance / 3. Administer prescribed pharmacotherapy.
diastolic augmentation ) a. ASA to suppress inflammatory process
Involves introduction of the intra – aortic b. Corticosteriods for more severe symptoms
balloon catheter via the femoral artery 4. Assist in pericardiocentesis if cardiac tamponade is
Intra Aortic Balloon Pump augments present.
5. Pericardiocentesis is aspiration of blood or fluid
diastole, resulting in increased perfusion
from pericardial sac.
of the coronary arteries and the
myocardium and a decrease in left
ventricular workload.
VI. CARDIAC TAMPONADE
The balloon is inflated during diastole, it
is deflated during sytole.
Also known as pericardial tamponade, is an emergency
Indications:
condition in which fluid accumulates in the pericardium
Cardiogenic shock
(the sac in which the heart is enclosed).
AMI
If the fluid significantly elevates the pressure on the heart
Unstable Angina
it will prevent the heart's ventricles from filling properly.
Open heart surgery
This in turn leads to a low stroke volume.
C. NURSING INTERVENTIONS The end result is ineffective pumping of blood, shock,
and often death.
1. Perform hemodynamic monitoring
2. Administer oxygen therapy A. PREDISPOSING FACTORS
3. Correct hypovolemia. Administer IV fluids as 1. Chest trauma ( blunt or penetrating )
ordered 2. Myocardial ruptured
4. Pharmacology: 3. Cancer
a. Vasodilators: Nitroglycerine 4. Pericarditis
b. Inotropic agents:Digitalis, Dopamine 5. Cardiac surgery ( first 24 – 48 hours )
c. Diuretics : Furosemide 6. Thrombolytic therapy
d. Sodium Bicarbonate, Relieve lactic acidosis
5. Monitor hourly urine output, LOC and arrhythmias B. SIGNS AND SYMPTOMS
6. Provide psychosocial support 1. Beck’s Triad
7. Decrease pulmonary edema Hypotension
a. Auscultate lung fields for crackles and wheezes Jugular venous distension
b. Note for dyspnea, cough , hemoptysis and Muffled heart sound
orthopnea 2. Pulsus paradoxus ( drop of at least 10 mmHg in
c. Monitor ABG for hypoxia and metabolic arterial BP on inspiration )
acidosis 3. Tachycardia
d. Place in fowler’s position to reduce venous 4. Breathlessness
return 5. Decrease in LOC
e. Administer during therapy as ordered:
Morphine sulfate to reduce venous
return.
Medical and Surgical Nursing 13 Abejo
14. Lecture Notes on Cardiovascular System
Prepared By: Mark Fredderick R Abejo R.N, MAN
C. NURSING INTERVENTIONS 3. Pulmonary embolism (char by chest pain and
dyspnea)
1. Administer oxygen 4. Pulmonic stenosis
2. Elevate head of bed, place pillow on the overbed 5. Left sided heart failure
table so that the patient can lean on it.
3. Bed rest B. SIGNS AND SYMPTOMS (Venous congestion)
4. Administer prescribed pharmacotherapy. 1. Jugular vein distention
c. ASA to suppress inflammatory process 2. Pitting edema
d. Corticosteriods for more severe symptoms 3. Ascites
5. Assist in pericardiocentesis and thoracotomy 4. Weight gain
6. Pericardiocentesis is aspiration of blood or fluid 5. Hepatosplenomegaly
from pericardial sac. 6. Jaundice
7. Pruritus/ urticaria
8. Esophageal varices
CONGESTIVE HEART FAILURE 9. Anorexia
10. Generalized body malaise
Inability of the heart to pump blood towards systemic C. DIAGNOSTICS
circulation 1. CXR – cardiomegaly
2. CVP – measures pressure in right atrium; N = 4-
I. LEFT-SIDED HEART FAILURE 10cc H2O
During CVP: trendelenburg to prevent
A. PREDISPOSING FACTORS pulmo embolism and to promote ventricular
1. 90% - Mitral valve stenosis filling
RHD Flat on bed post CVP, check CVP readings
Inflammation of mitral valve Hypovolemia – fluid challenge
Anti-streptolysin O titer (ASO) – 300 todd Hypervolemia – diuretics (loop)
units 3. Echocardiography – reveals enlarged heart chamber
Penicillin, PASA, steroids Muffled heart sounds cardiomyopathy
Aging Cyanotic heart diseases
2. MI TOF “tet” spells cyanosis with
3. IHD hypoxemia
4. HPN Tricuspid valve stenosis
5. Aortic valve stenosis Transposition of aorta
Acyanotic
B. SIGNS AND SYMPTOMS PDA – machine-like murmur
1. Pulmonary edema/congestion DOC: indomethacin SE: corneal
Dyspnea, PND (awakening at night d/t cloudiness
difficulty in breathing), 2-3 pillow orthopnea 4. Liver enzymes
Productive cough (blood tinged) SGPT up
Rales/crackles SGOT up
Bronchial wheezing
Frothy salivation D. NURSING MANAGEMENT
2. Pulsus alternans (A unique pattern during which the
amplitude of the pulse changes or alternates in size Goal: increase myocardial contraction increase CO;
with a stable heart rhythm.)This is common in Normal CO is 3-6L/min; N stroke volume is 60-70ml/h2o
severe left ventricular dysfunction.)
3. Anorexia and general body malaise 1. Administer medications as ordered
4. PMI displaced laterally, cardiomegaly Cardiac glycosides
5. S3 (ventricular gallop) Digoxin (N=.5-1.5, tox=2)
Tox: Anorexia, N&V; A: Digibind
C. DIAGNOSTICS Digitoxin – given if (+) ARF; metabolized
1. CXR – cardiomegaly in liver and not in kidneys
2. PAP – pulmonary arterial pressure Loop diuretics
Measures pressure in right ventricle Lasix – IV push, mornings
Reveals cardiac status Bronchodilators
3. PCWP – pulmonary capillary wedge pressure Aminophylline (theophylline)
Measures end-systolic and end-diastolic Tachycardia, palpitations
pressure (elevated)
CNS hyperactivity, agitation
Done through cardiac catheterization (Swan-
Narcotic analgesics
Ganz)
Morphine sulfate – induces vasodilation
4. Echocardiograph – reveals enlarged heart chamber
Vasodilators
5. ABG analysis reveals elevated PCO2 and decreased
NTG and ISDN
PO2 (respiratory acidosis) hypoxemia and
Anti-arrhythmic agents
cyanosis
Lidocaine (SE: dizziness and
Tracheostomy for severe respiratory distress and laryngospasm confusion)
performed at bedside within 10-15 minutes Bretyllium
YOU DON’T GIVE BETA-BLOCKERS TO
CVP reveals fluid status; Normal = 4-10cm H2o; right atrium THESE PATIENTS
PAP – cardiac status; left atrium 2. Administer O2 inhalation at 3-4 L/minute via NC as
ALLEN’S test – collateral circulation ordered high flow
Cardiac Tamponade: pulsus paradoxus, muffled heart sounds, HPN
3. High fowler’s, 2-3 Pillows
4. Restrict Na and fluids
II. RIGHT SIDED HEART FAILURE
5. Monitor strictly VS and IO and Breath Sounds
6. Weigh pt daily and assess for pitting edema
A. PREDISPOSING FACTORS
7. abdominal girth daily and notify MD
1. Tricuspid valve stenosis
8. provide meticulous skin care
2. COPD
Medical and Surgical Nursing 14 Abejo