134398619 1-fluid-volume-excess-chronic-renal-failure-nursing-care-plans

This patient has been diagnosed with renal failure due to decreased glomerular filtration rate and sodium retention. Objective findings include edema, hypertension, weight gain, pulmonary congestion, oliguria, distended jugular veins, and changes in mental status. The nursing diagnosis is fluid volume excess related to decreased glomerular filtration rate and sodium retention impairing the kidneys' ability to filter fluids and excrete excess sodium. Short term goals are for the patient to demonstrate behaviors to monitor fluid status and reduce recurrence of fluid excess within 4-8 hours. Long term goals are for the patient to have stabilized fluid volume as evidenced by balanced intake/output, normal vital signs, stable weight, and freedom from edema signs within 3 days with nursing

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Similar to 134398619 1-fluid-volume-excess-chronic-renal-failure-nursing-care-plans
Similar to 134398619 1-fluid-volume-excess-chronic-renal-failure-nursing-care-plans (20)
134398619 1-fluid-volume-excess-chronic-renal-failure-nursing-care-plans
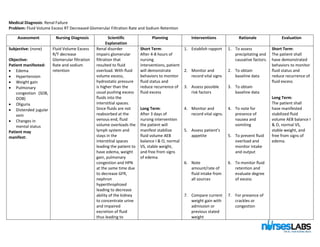
- 1. Medical Diagnosis: Renal Failure Problem: Fluid Volume Excess RT Decreased Glomerular Filtration Rate and Sodium Retention Assessment Nursing Diagnosis Scientific Explanation Planning Interventions Rationale Evaluation Subjective: (none) Objective: Patient manifested: Edema Hypertension Weight gain Pulmonary congestion (SOB, DOB) Oliguria Distended jugular vein Changes in mental status Patient may manifest: Fluid Volume Excess R/T decrease Glomerular filtration Rate and sodium retention Renal disorder impairs glomerular filtration that resulted to fluid overload. With fluid volume excess, hydrostatic pressure is higher than the usual pushing excess fluids into the interstitial spaces. Since fluids are not reabsorbed at the venous end, fluid volume overloads the lymph system and stays in the interstitial spaces leading the patient to have edema, weight gain, pulmonary congestion and HPN at the same time due to decrease GFR, nephron hyperthrophized leading to decrease ability of the kidney to concentrate urine and impaired excretion of fluid thus leading to Short Term: After 4-8 hours of nursing interventions, patient will demonstrate behaviors to monitor fluid status and reduce recurrence of fluid excess Long Term: After 3 days of nursing intervention the patient will manifest stabilize fluid volume AEB balance I & O, normal VS, stable weight, and free from signs of edema. 1. Establish rapport 2. Monitor and record vital signs 3. Assess possible risk factors 4. Monitor and record vital signs. 5. Assess patient’s appetite 6. Note amount/rate of fluid intake from all sources 7. Compare current weight gain with admission or previous stated weight 1. To assess precipitating and causative factors. 2. To obtain baseline data 3. To obtain baseline data 4. To note for presence of nausea and vomiting 5. To prevent fluid overload and monitor intake and output 6. To monitor fluid retention and evaluate degree of excess 7. For presence of crackles or congestion Short Term: The patient shall have demonstrated behaviors to monitor fluid status and reduce recurrence of fluid excess Long Term: The patient shall have manifested stabilized fluid volume AEB balance I & O, normal VS, stable weight, and free from signs of edema.
- 2. oliguria/anuria. 8. Auscultate breath sounds 9. Record occurrence of dyspnea 10. Note presence of edema. 11. Measure abdominal girth for changes. 12. Evaluate mentation for confusion and personality changes. 13. Observe skin mucous membrane. 14. Change position of client timely. 15. Review lab data like BUN, Creatinine, Serum electrolyte. 16. Restrict sodium and fluid intake if 8. To evaluate degree of excess 9. To determine fluid retention 10. May indicate increase in fluid retention 11. May indicate cerebral edema. 12. To evaluate degree of fluid excess. 13. To prevent pressure ulcers. 14. To monitor fluid and electrolyte imbalances 15. To lessen fluid retention and overload. 16. To monitor kidney function
- 3. indicated 17. Record I&O accurately and calculate fluid volume balance 18. Weigh client 19. Encourage quiet, restful atmosphere. 20. Promote overall health measure. and fluid retention. 17. Weight gain indicates fluid retention or edema. 18. Weight gain may indicate fluid retention and edema. 19. To conserve energy and lower tissue oxygen demand. 20. To promote wellness.