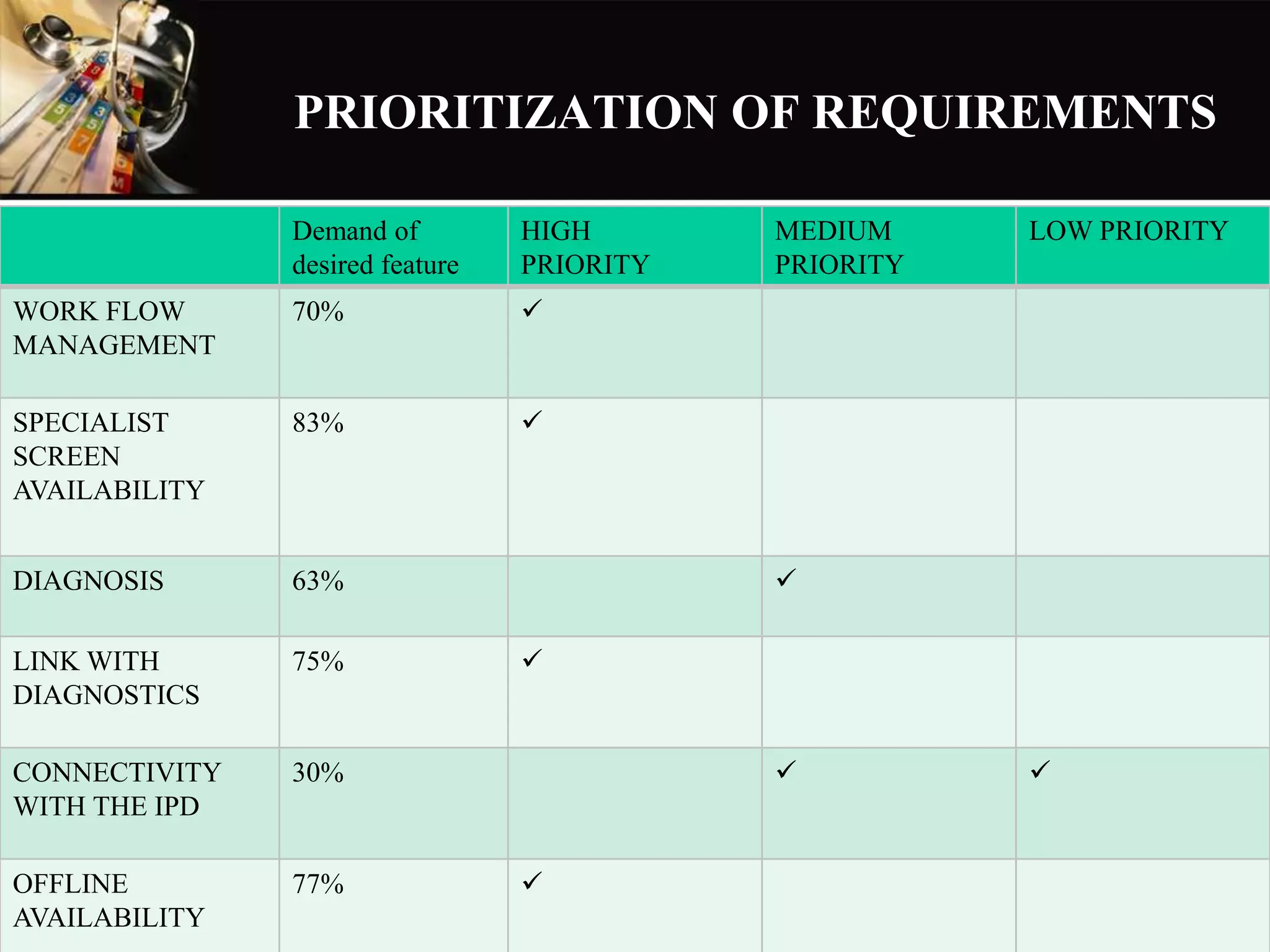
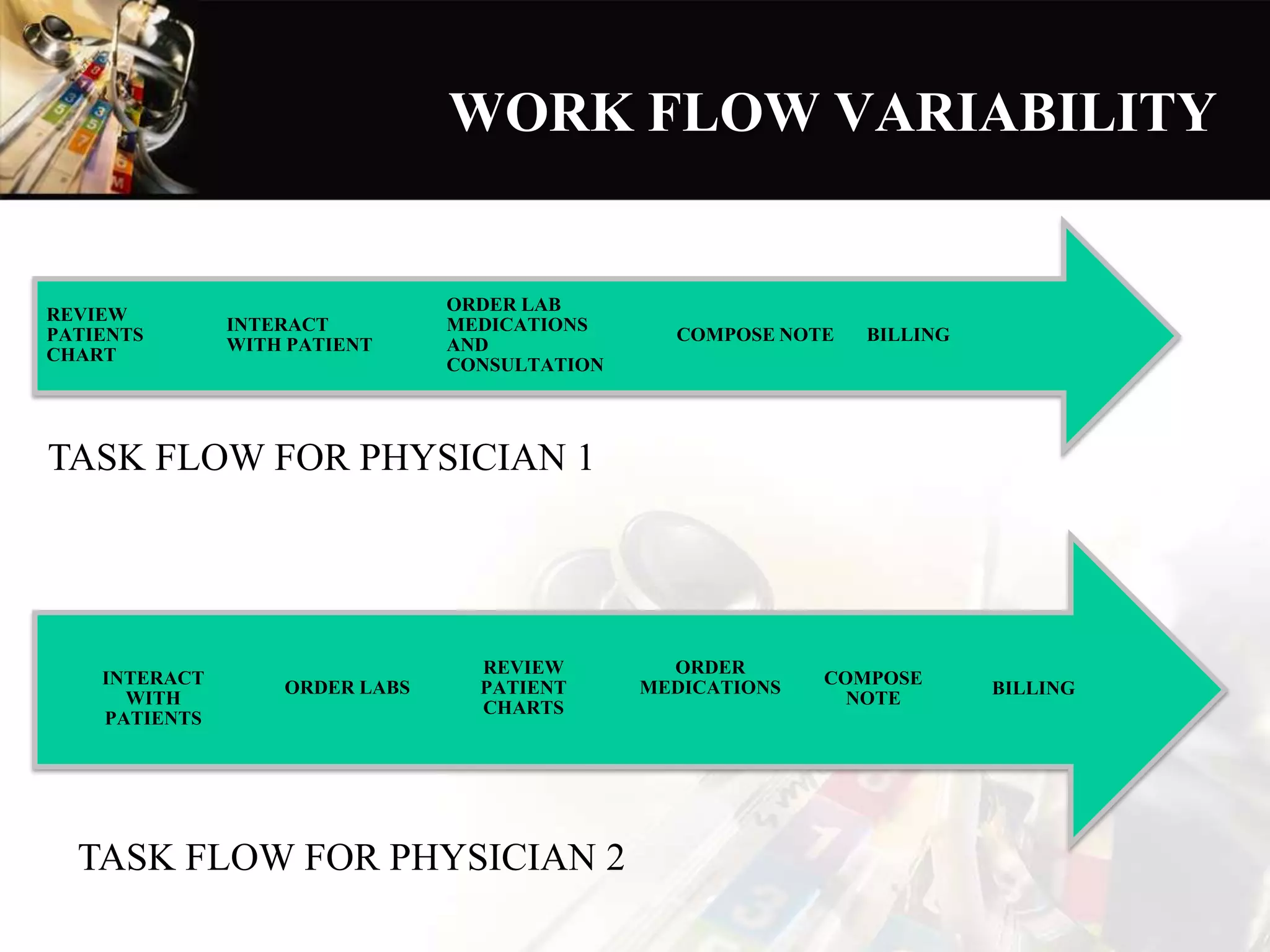
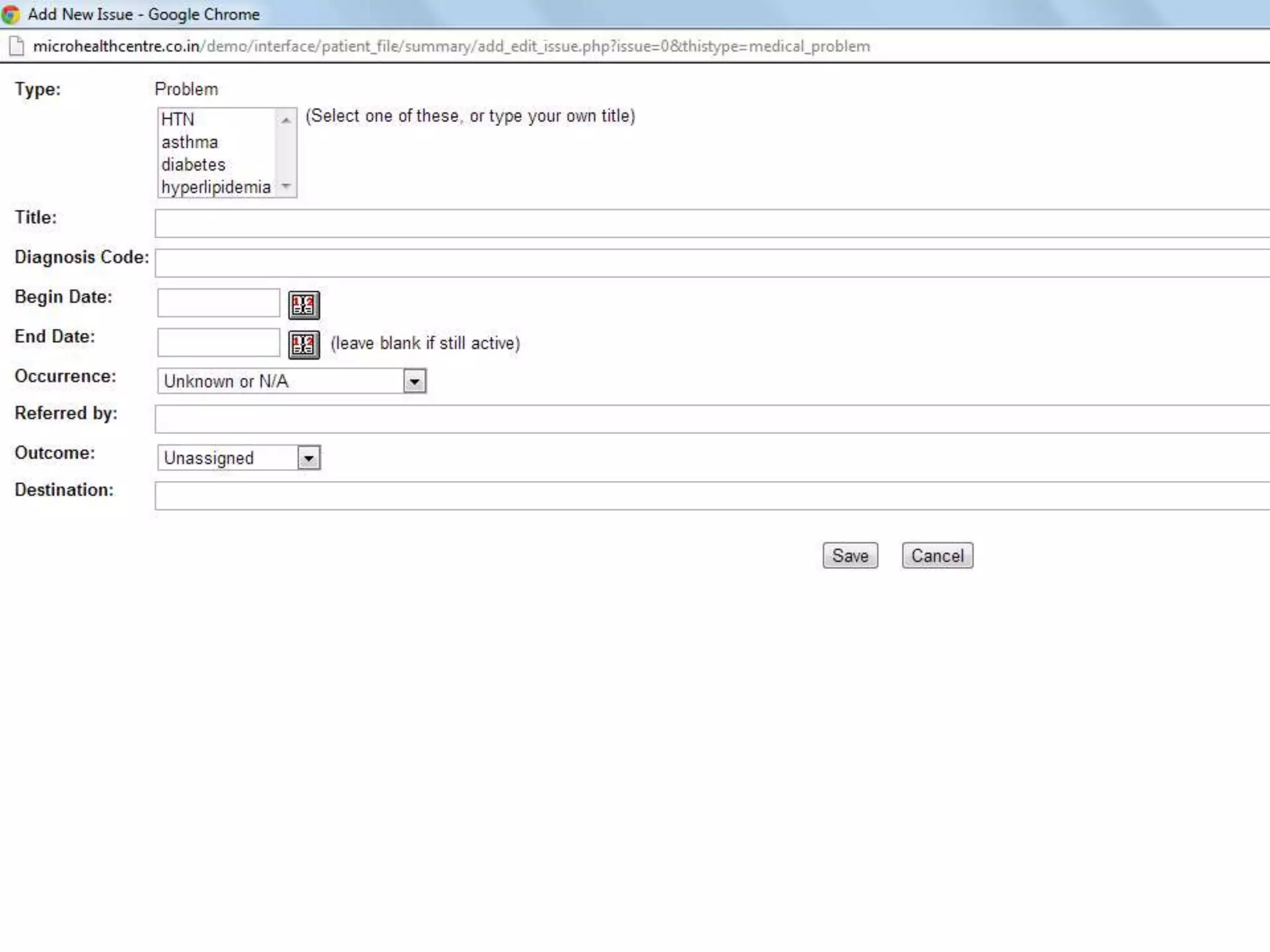
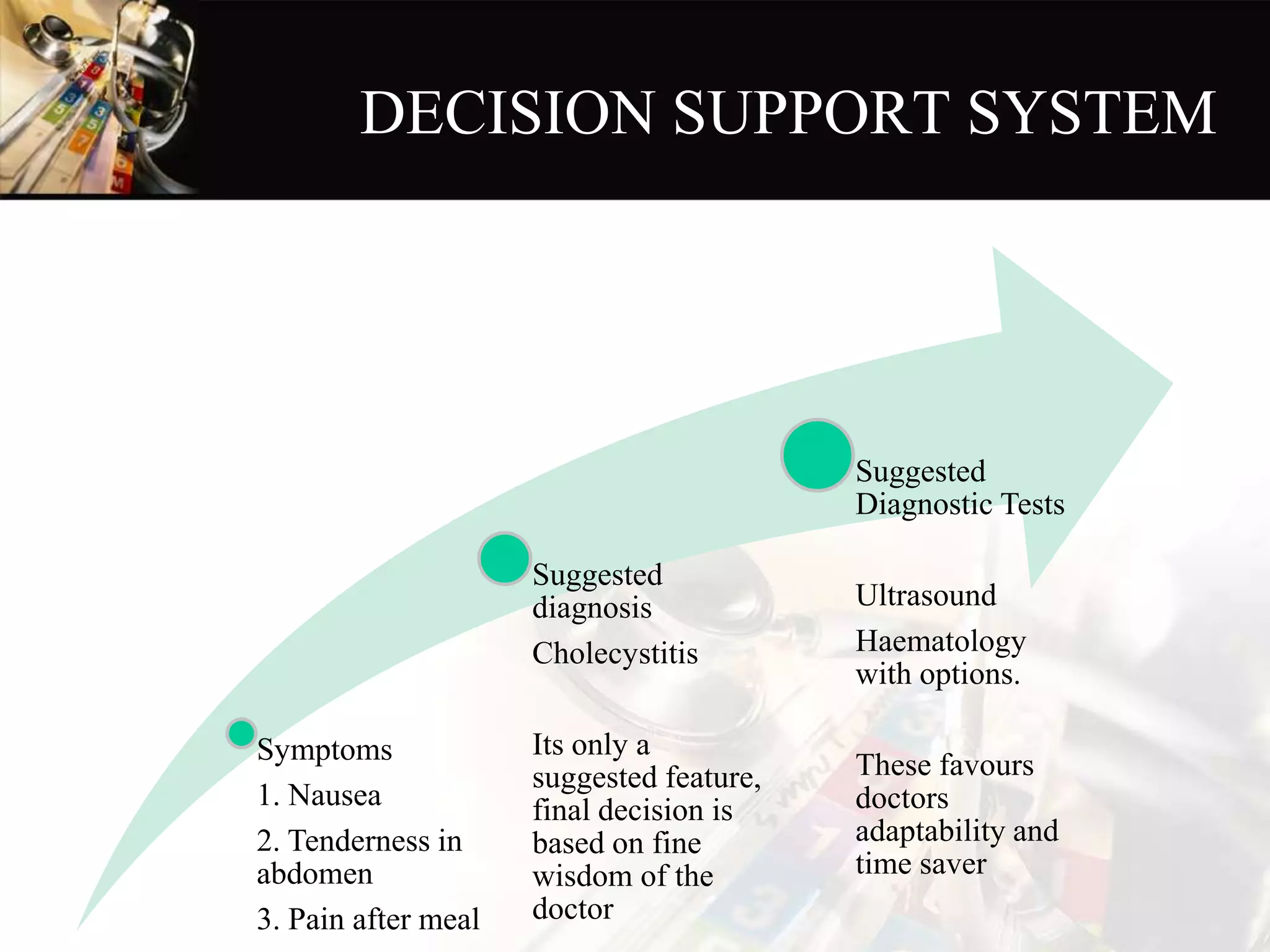
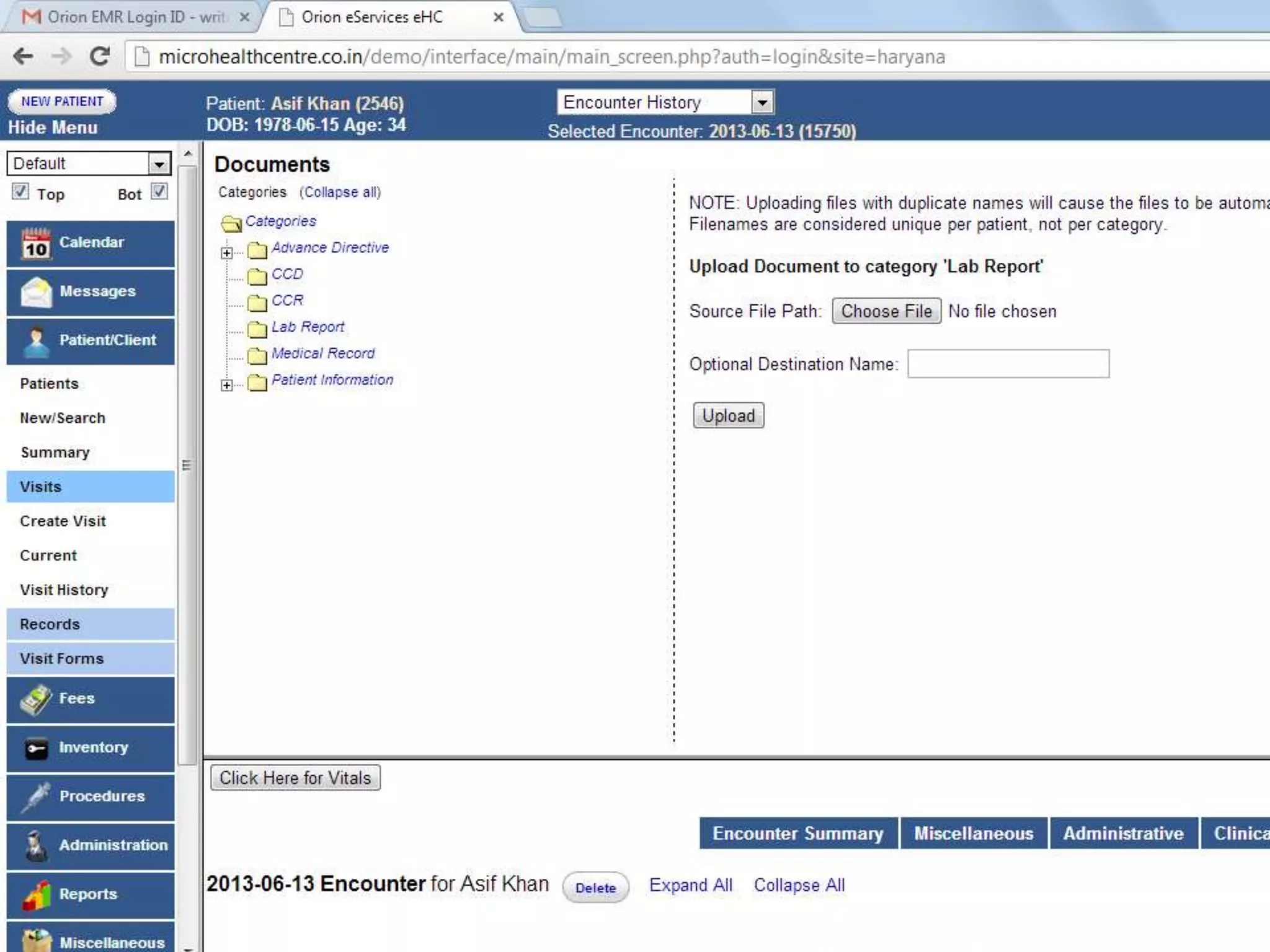
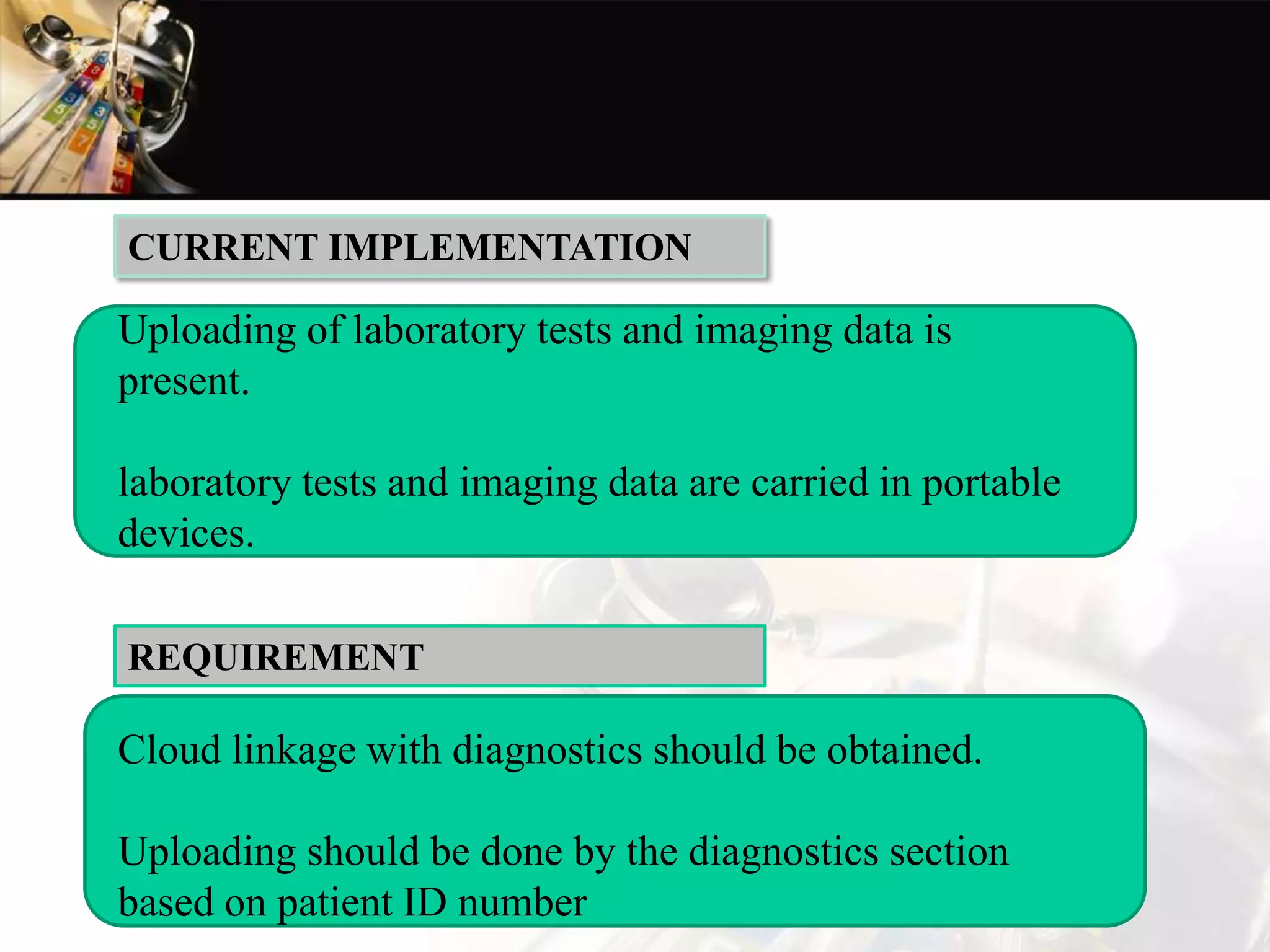
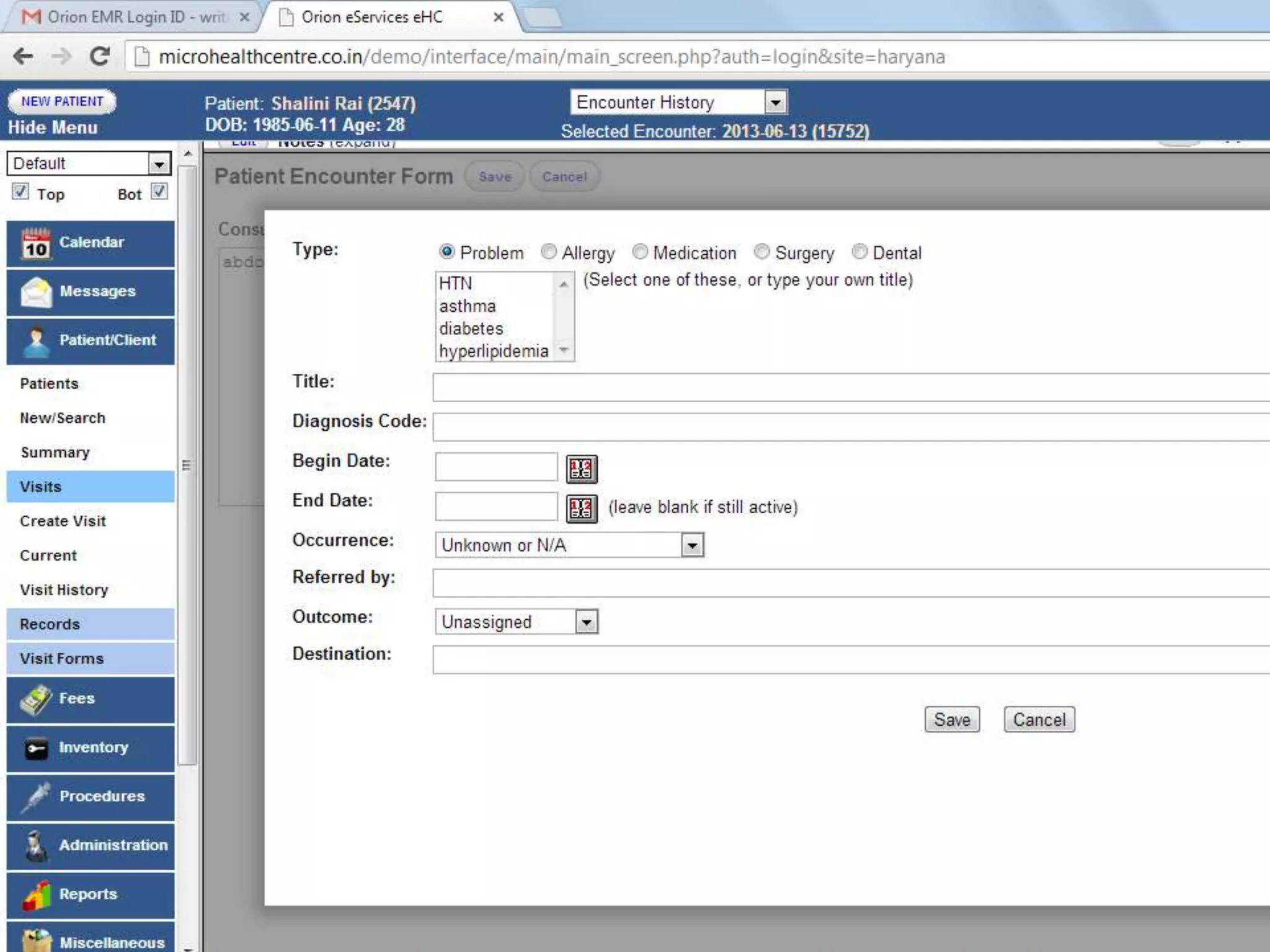
The document outlines requirements for customizing an electronic medical records (EMR) system developed by HP. It describes conducting interviews and questionnaires with doctors to gather feedback on needed improvements. Key areas identified include workflow management, specialist screens, diagnosis features, linking to diagnostic labs, connectivity to hospitalization records, and offline availability. The document makes recommendations for customizing the EMR for different specialties and adding features like integrated decision support, online/offline functionality, and compliance with medical legal standards.