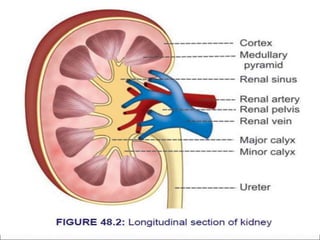
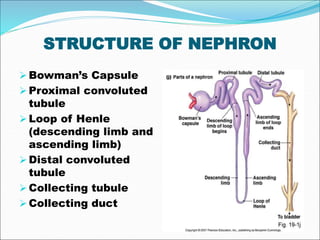
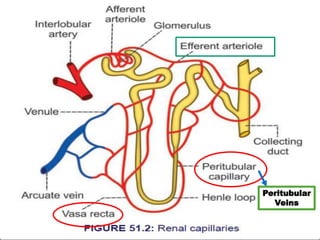
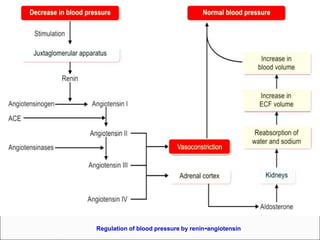
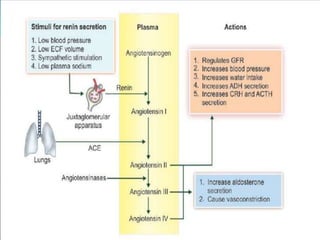
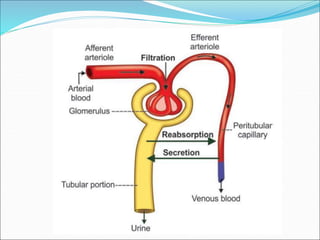
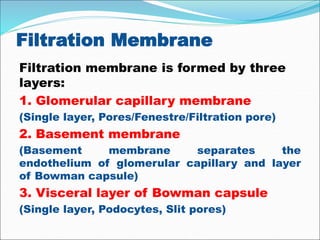
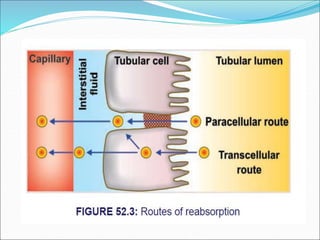
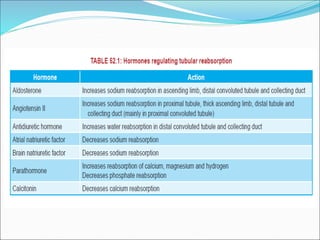
The document details the excretion processes in the human body, focusing on various organs such as the digestive system, lungs, skin, liver, and kidneys. It describes the structure and function of nephrons, the formation of urine through glomerular filtration, tubular reabsorption, and secretion, and the regulation of these processes by hormonal mechanisms. Additionally, it addresses the implications of renal failure, including acute and chronic conditions.