Downloaded 285 times

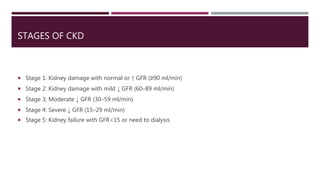
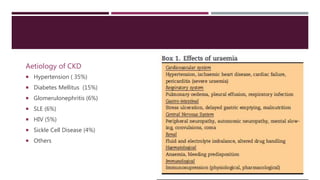
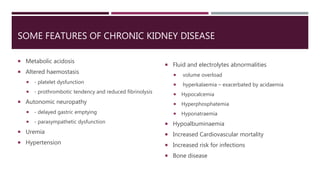

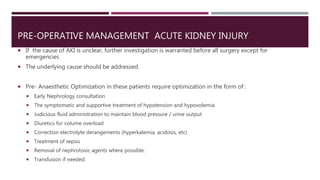

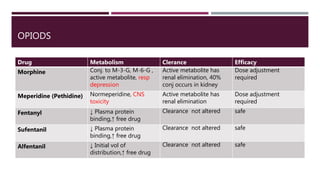
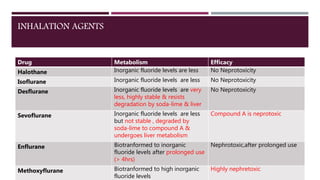
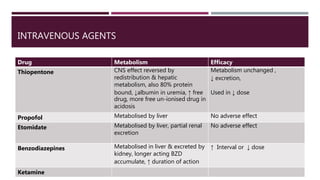
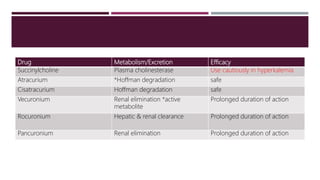
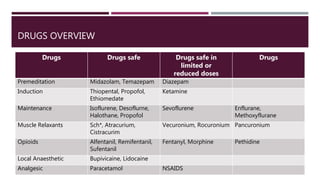
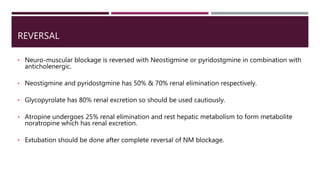
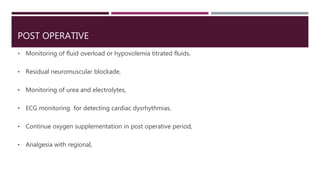


The document discusses renal impairment in anesthesia, including acute kidney injury (AKI) and chronic kidney disease (CKD). It covers the definition, causes, and staging of AKI and CKD. Pre-operative management of patients with renal impairment focuses on optimizing fluid, electrolyte and acid-base status. Intra-operatively, reduced doses of medications may be needed due to impaired drug clearance. Regional anesthesia offers advantages over general anesthesia when possible. Careful post-operative monitoring of fluid balance and renal function is also emphasized.


















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







