Downloaded 167 times
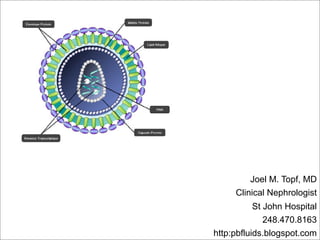
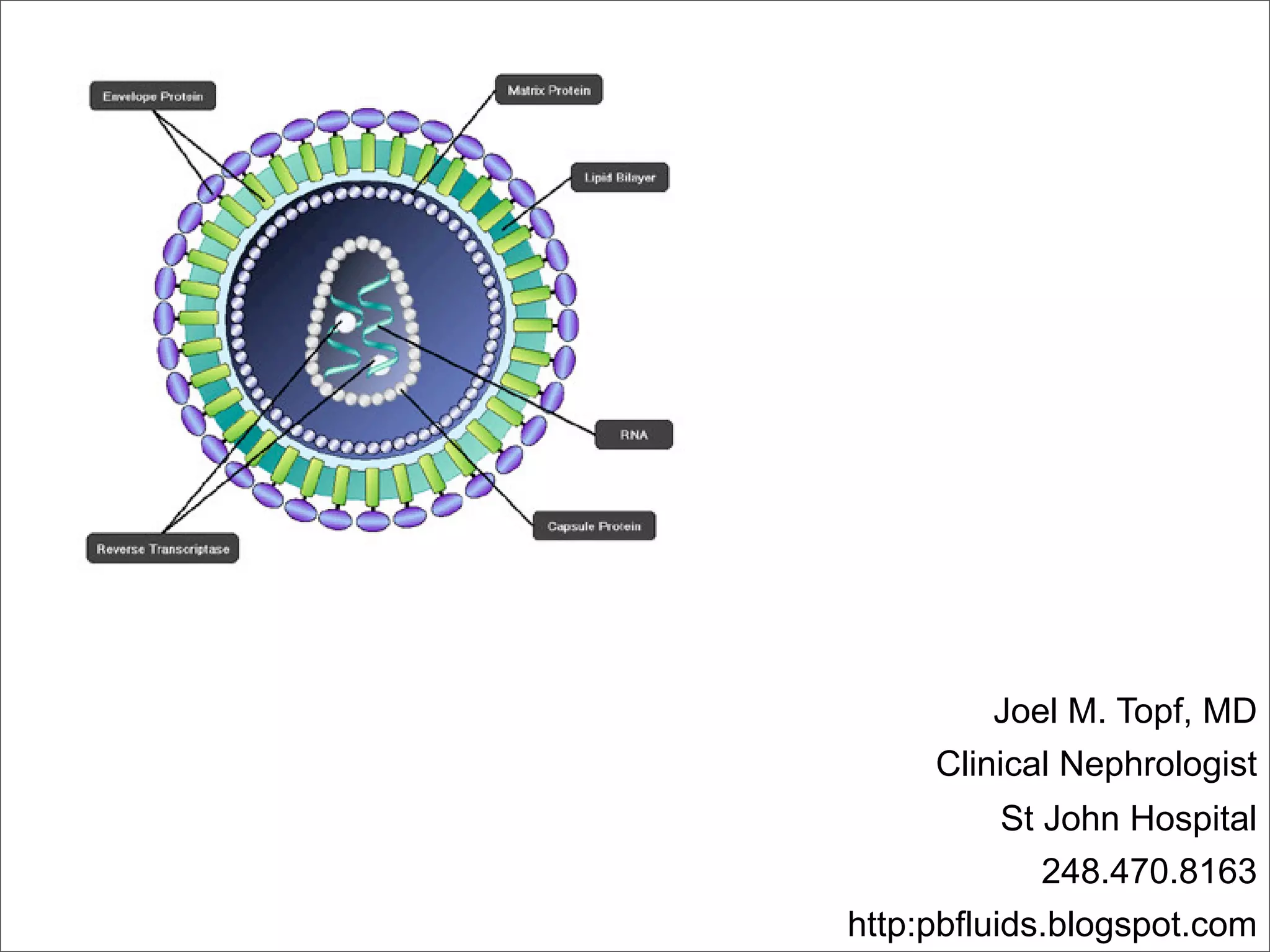

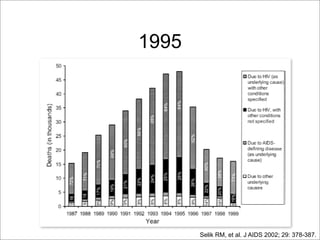
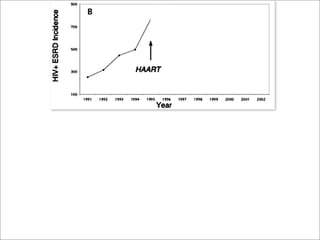
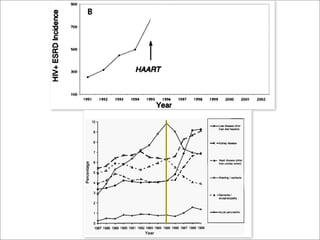
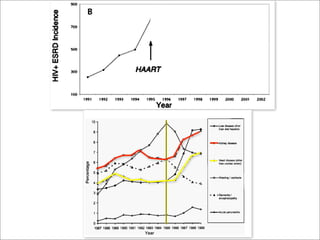
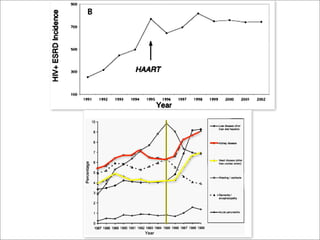




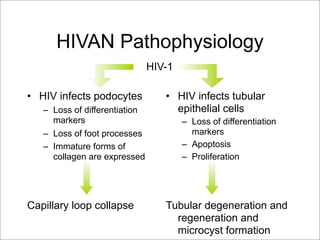
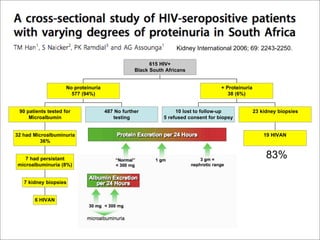
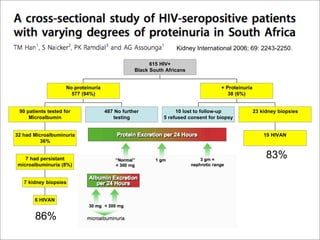
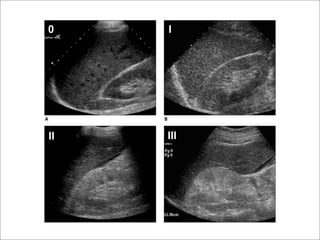
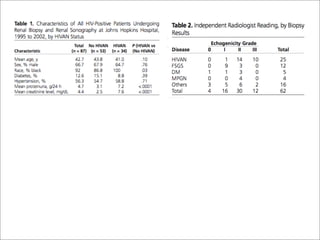
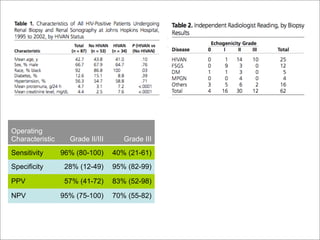
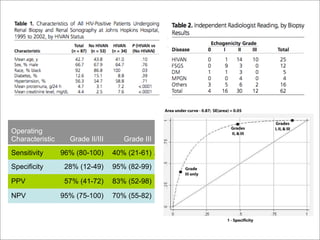
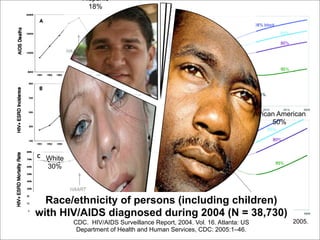
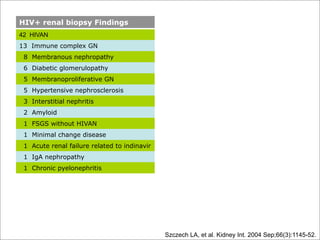
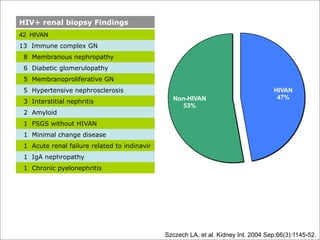
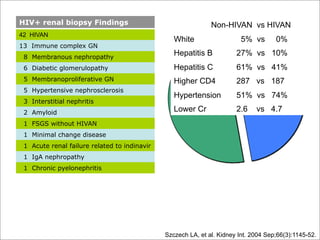
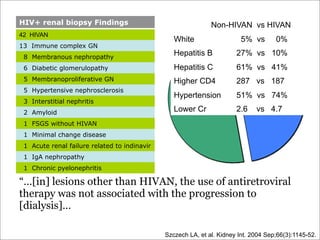

This document discusses HIV and its impact on the kidney. It begins with biographical information about the author, Joel M. Topf, MD, a clinical nephrologist. It then covers topics like the history of HIV, the identification of HIVAN (HIV-associated nephropathy) as a renal manifestation of HIV, characteristics of HIVAN such as its association with African Americans, and changes in HIV renal disease over time with the introduction of antiretroviral therapy. It provides data on prevalence of HIVAN from renal biopsies and risk factors associated with HIVAN compared to other kidney conditions in HIV+ patients.










































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)












