Downloaded 186 times




















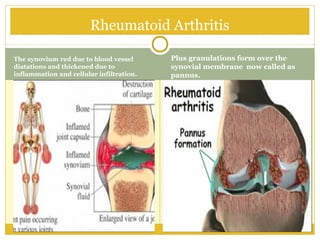



































































Rheumatoid arthritis (RA) is an autoimmune disease that causes chronic inflammation of the joints. It can affect people of all ages but typically occurs between ages 35-50 and affects women more than men. RA causes inflammation of the synovial membranes around joints which can lead to pain, stiffness, swelling, and over time, destruction of cartilage and bone. While the exact cause is unknown, genetic and environmental factors are believed to play a role. Treatment focuses on reducing inflammation and preventing further joint damage through medications and physical therapy.























































































