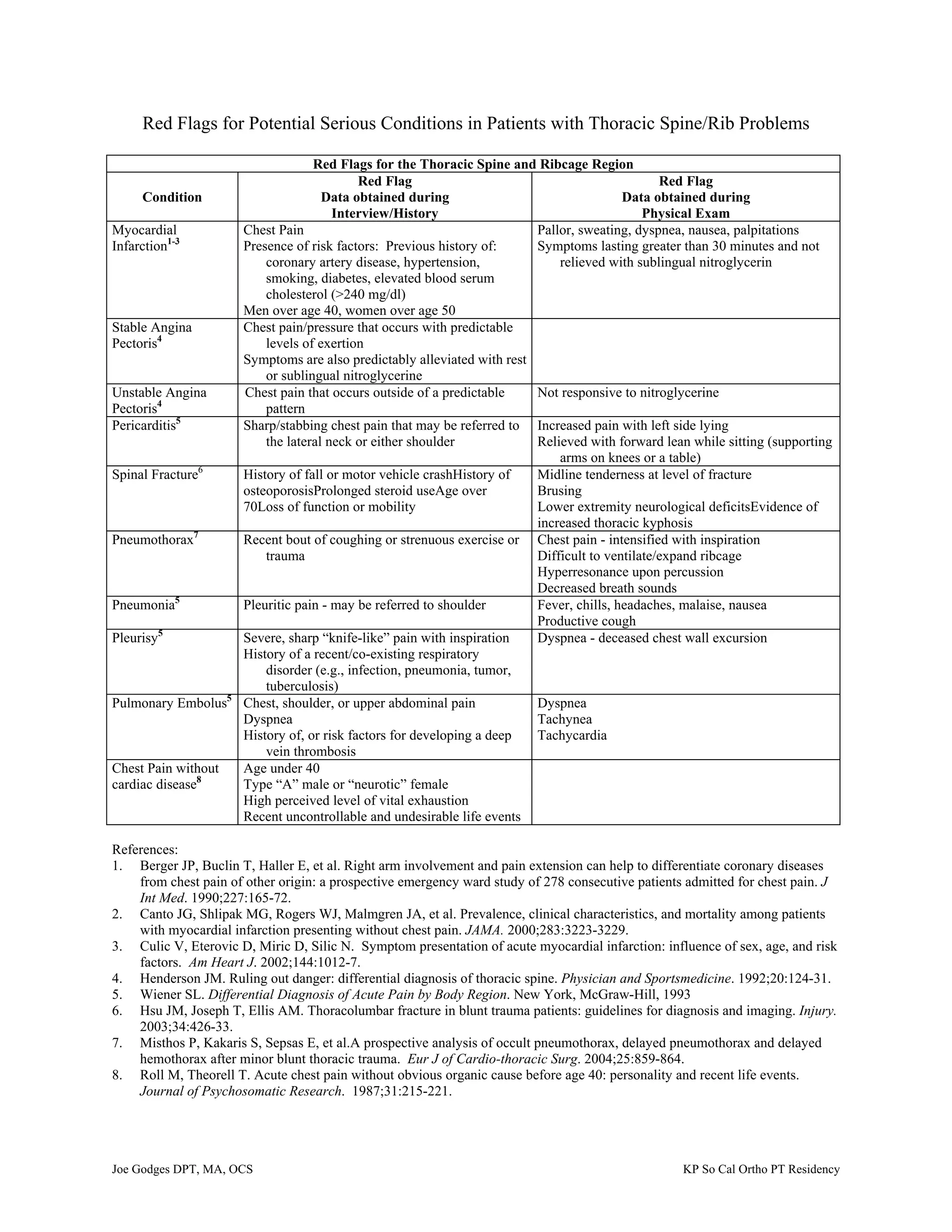
This document lists potential serious medical conditions that can present with thoracic spine or rib problems, along with associated red flags from patient history and physical exam. It identifies red flags for conditions like myocardial infarction, angina, pericarditis, spinal fracture, pneumothorax, pneumonia, pleurisy, pulmonary embolism, and chest pain without cardiac causes. Red flags include things like certain types of chest pain, dyspnea, risk factors, fever, cough, and physical exam findings related to each condition. Differentiating these conditions is important for guiding appropriate medical management.











































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)










![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
