Downloaded 90 times
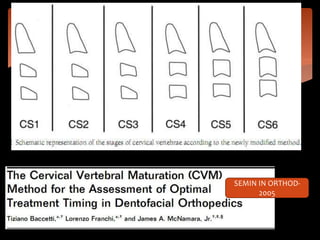


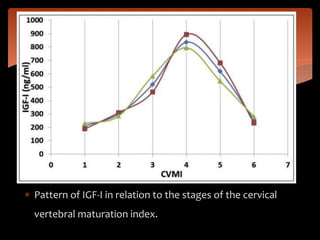


The document summarizes recent advances in skeletal maturity studies. It discusses modified methods to assess skeletal maturity including the modified cervical vertebral maturation method and modified MP3 staging. It also reviews recent literature on the relationship between skeletal maturity and factors like maxillary canine eruption, serum DHEAS, PTHrP, and IGF-1 levels. A variety of methods have been used to better understand the biological mechanisms influencing craniofacial growth and skeletal development.





![FACEMASK CHINCUP SEMINAR[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/facemaskchincupseminar1-230916061625-e0964de8-thumbnail.jpg?width=640&height=640&fit=bounds)




























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)












