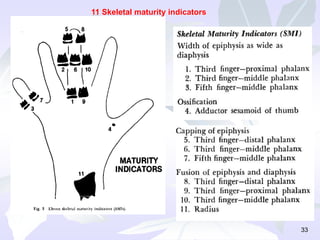
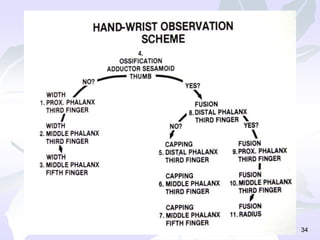
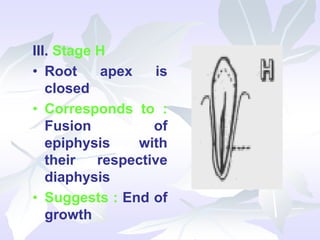
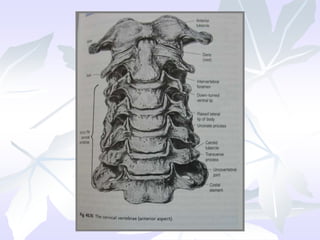
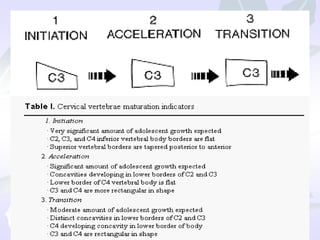
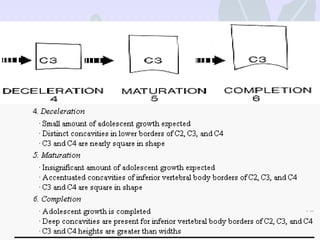
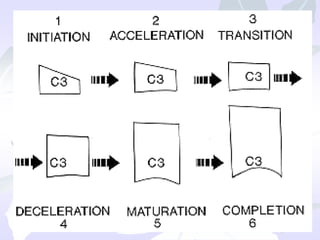
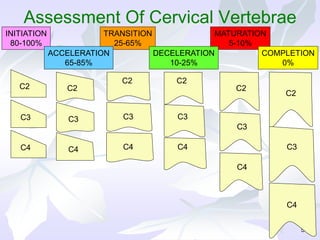
This document discusses various skeletal maturity indicators used to assess skeletal age and predict growth spurts. It describes methods using hand-wrist radiographs, tooth mineralization of the mandibular canine, and cervical vertebrae morphology. For hand-wrist radiographs, it outlines the anatomy and several methods to evaluate skeletal maturity stages based on ossification of carpals, metacarpals, and phalanges. Tooth mineralization focuses on mandibular canine root development. Cervical vertebrae maturation is assessed using morphological changes that occur in predictable sequences.