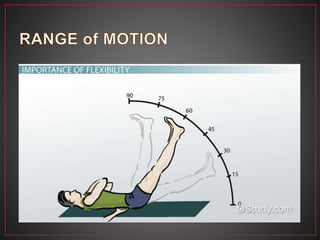
Range of motion (ROM) refers to the extent of movement possible at a joint and is influenced by the muscles that cross that joint. There are three types of ROM: passive ROM, which is movement produced by an external force with no voluntary muscle contraction; active ROM, which involves active muscle contraction; and active-assistive ROM, which combines active contraction with external assistance. Passive ROM is used when a patient cannot actively move and aims to maintain joint mobility and flexibility. Active ROM is used when a patient can contract muscles to move and helps build coordination, circulation, and strength. The type of ROM used depends on a patient's abilities and healing status.