Radiotherapy for Seminoma
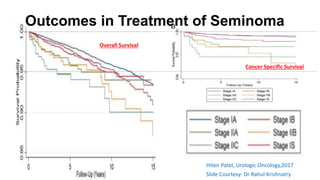
- Seminoma accounts for over 60% of testicular germ cell tumors with an incidence of 0.95 per 100,000.
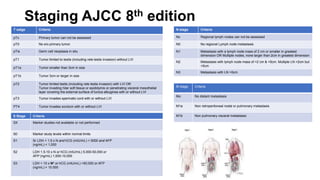
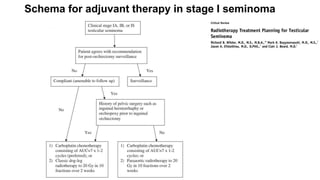
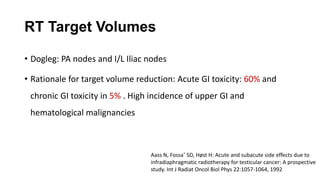
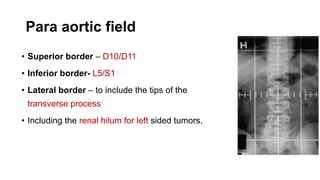
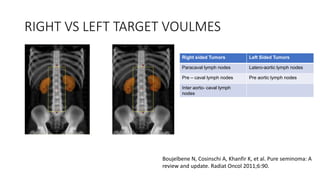
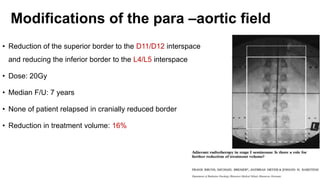
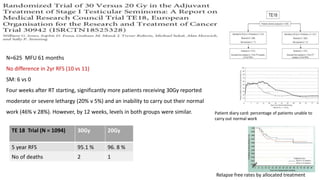
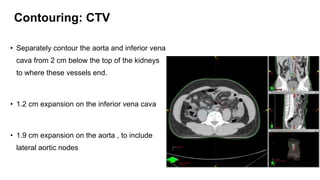
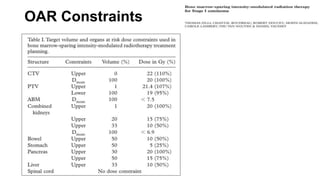
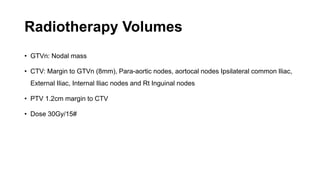
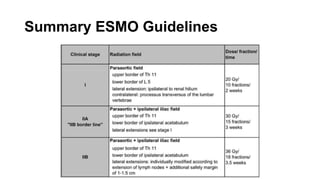
- For stage I seminoma, prophylactic radiation to the para-aortic lymph nodes is the standard of care to reduce the risk of recurrence.
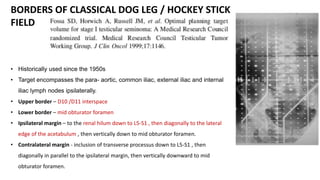
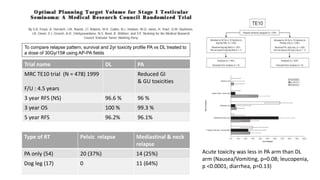
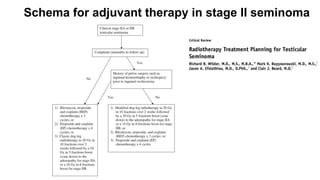
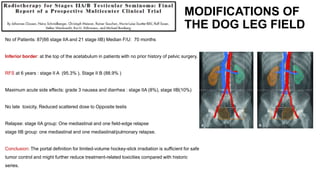
- For stage IIA/IIB seminoma, radiotherapy to the para-aortic, iliac, and inguinal lymph nodes is recommended, with 30Gy to the whole field and a 10Gy boost for stage IIA and 36Gy total for stage IIB.
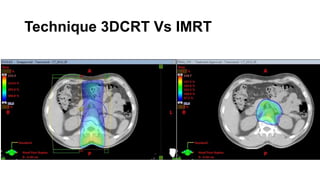
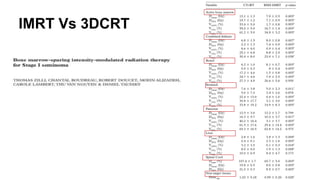
- Intensity modulated radiation therapy (IMRT) allows for improved sparing of
















![Rrecent advances in linear accelerators [MR linac]](https://cdn.slidesharecdn.com/ss_thumbnails/icroproadvance2021-recentadvancesinlinearaccelerators-211201040416-thumbnail.jpg?width=640&height=640&fit=bounds)

















































