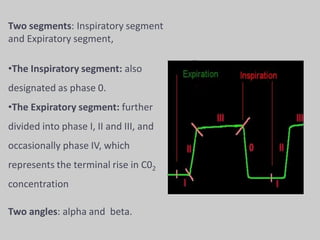
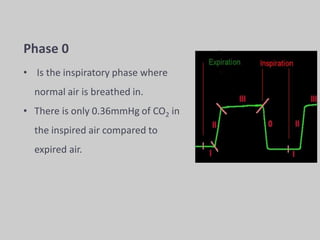
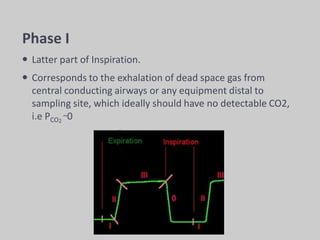
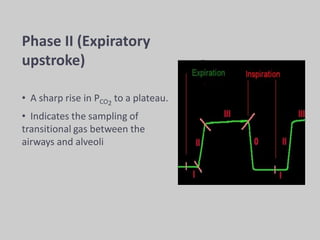
The document discusses pulse oximetry and capnography, emphasizing their importance in non-invasive monitoring of oxygen saturation and carbon dioxide levels, respectively. It outlines the principles and technology behind pulse oximeters and capnometers, including their applications in anesthesia and critical care, as well as common limitations and alternatives to these monitoring methods. The text also highlights the significance of integrating both techniques to enhance patient safety and reduce anesthesia-related mishaps.

![O2 content of arterial blood is,
CaO2 = Oxygen bound to hemoglobin + O2 dissolved in plasma
CaO2 = [1.36 × Hb × HbO % (SpO2)] + [0.003 × PaO2].
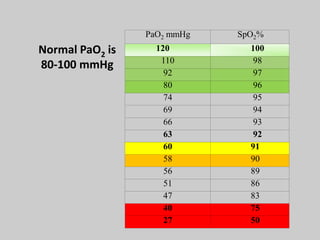
Pulse oximeter provides a non
invasive measurement of
arterial hemoglobin saturation,
a variable that is directly
related to oxygen content of
arterial
blood..](https://image.slidesharecdn.com/pulseoximetryandcapnographypptdharmaraj-240706002352-be1ad8e1/85/pulseoximetry-and-capnography-ppt-dharmaraj-pdf-12-320.jpg)