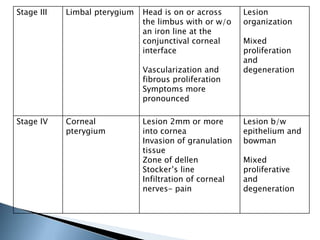
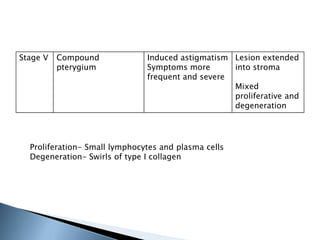
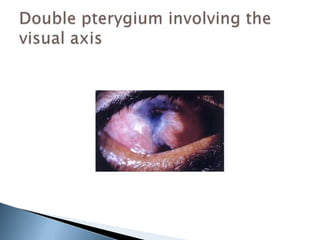
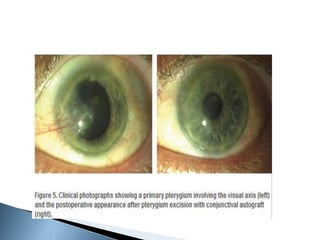
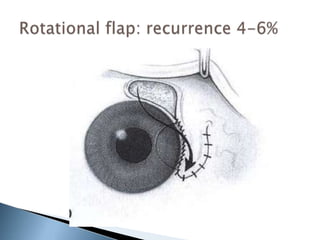
Pterygium is a non-malignant growth of fibrovascular tissue that arises from the conjunctiva and extends onto the cornea. It is more common in hot, dry, and dusty climates with high UV exposure. Prolonged UV exposure causes changes in the conjunctiva that promote angiogenesis and abnormal cell growth. Surgical excision is often required for pterygium that cause visual symptoms or encroach significantly onto the cornea. Recurrence after surgery is common due to residual stem cells and continued exposure to risk factors like UV light. Various adjunctive treatments can help reduce recurrence rates, such as conjunctival autografting, mitomycin C, and post-operative steroids.