Downloaded 283 times


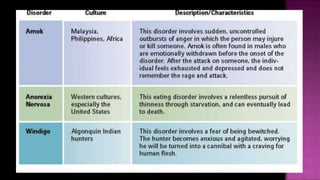
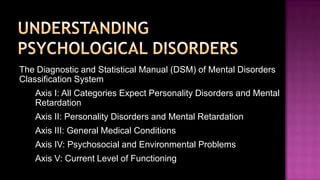



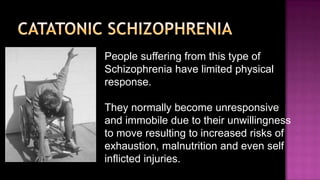

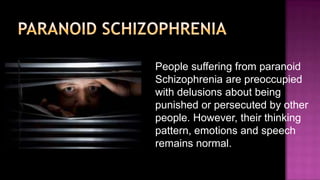
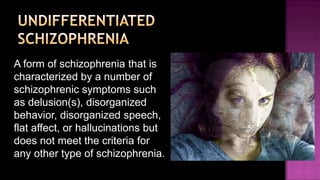


Psychological disorders can be understood from biological, psychological, and socio-cultural perspectives. They are classified in the DSM and include anxiety disorders like generalized anxiety disorder, panic disorder, and PTSD. Mood disorders involve disturbances in mood like depression and bipolar disorder. Schizophrenia impacts thinking, perception, communication and behavior with symptoms like delusions and hallucinations. Personality disorders are chronic maladaptive patterns grouped into odd/eccentric, dramatic/emotionally problematic, and chronic fearfulness clusters which include paranoid, antisocial, avoidant, and obsessive-compulsive types.





















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








