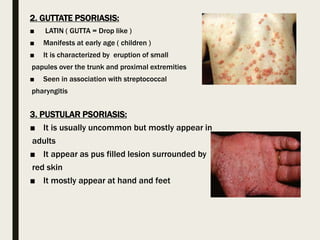
This document provides information about group members studying psoriasis and summarizes key points about the disease. It discusses the etiology, pathogenesis, clinical manifestations, types, diagnosis and first-line and second-line treatment options for psoriasis. Psoriasis is characterized by thickened, scaly skin plaques and is caused by an immune system problem involving T cells. Common types include plaque, guttate and pustular psoriasis. Treatment involves topical corticosteroids, vitamin D analogs and systemic drugs like methotrexate, cyclosporine and biologics that target T cells and inflammation.