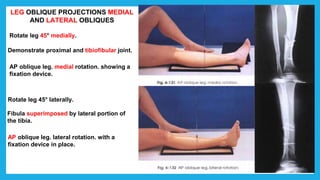
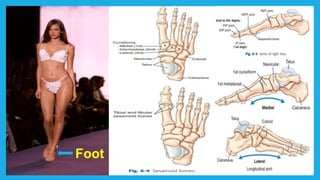
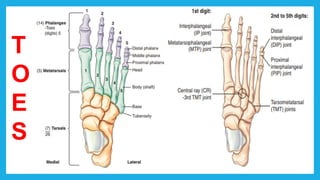
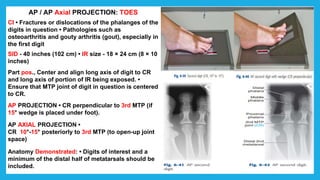
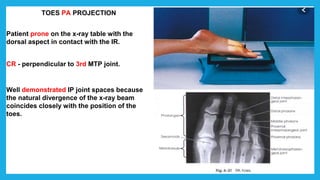
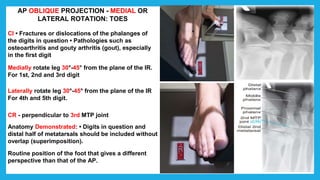
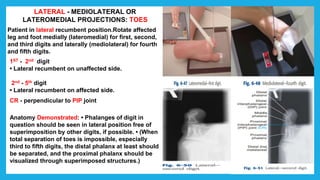
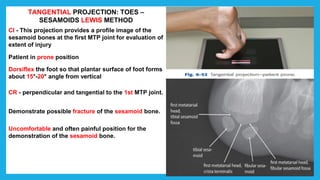
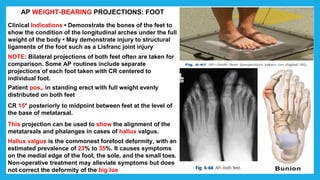
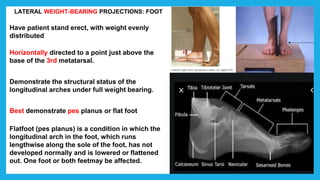
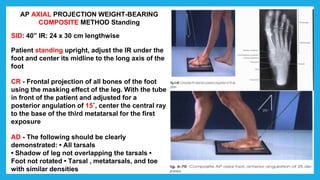
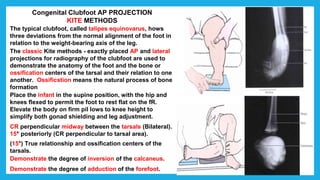
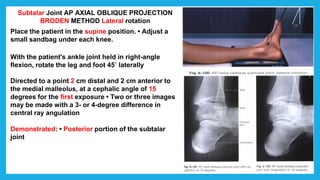
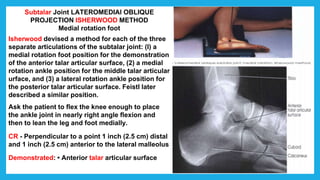
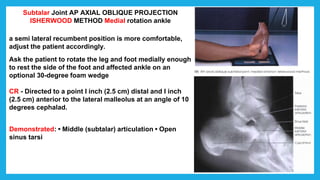
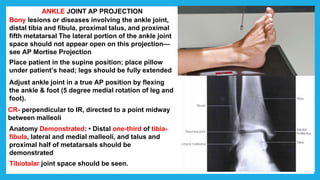
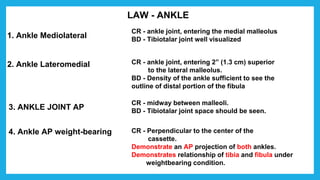
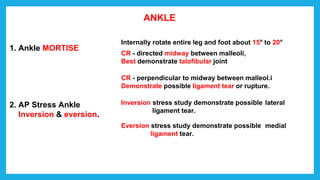
The document provides positioning and technical instructions for taking radiographs of various parts of the lower limb, including the foot, leg, toes, and calcaneus. It describes placing the patient in different positions such as supine, prone, lateral recumbent, and standing. It provides details on angling the central ray and image receptor to demonstrate specific anatomical structures like bones and joints. The instructions aim to clearly show fractures, dislocations, and other pathologies in different projections.