Download to read offline

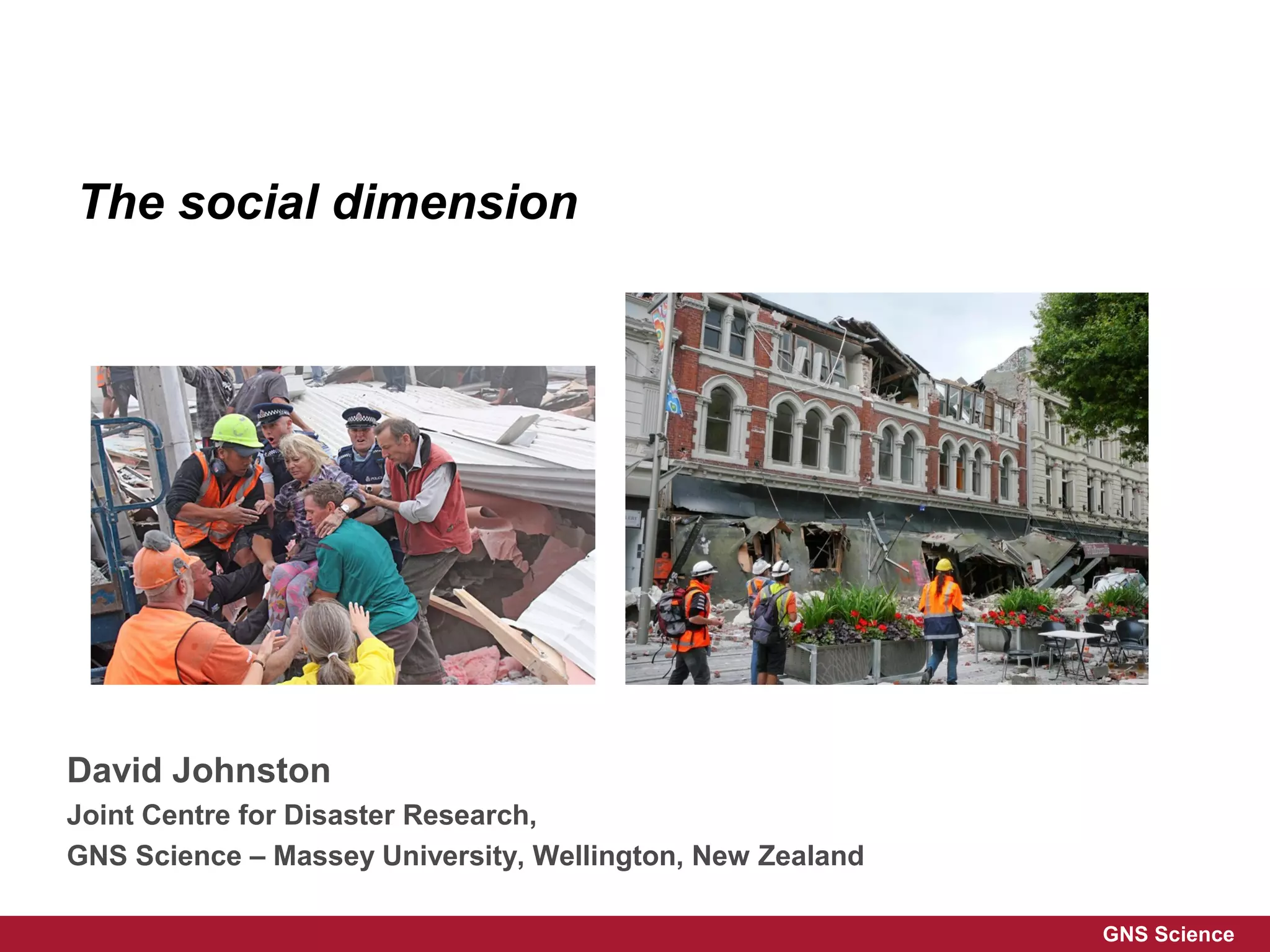
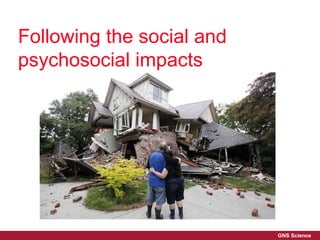
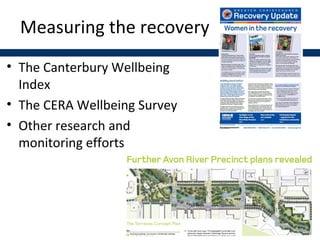
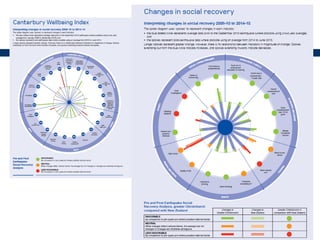

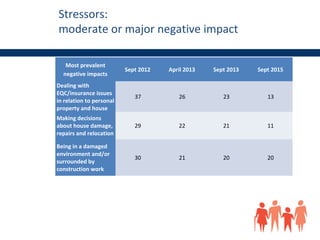
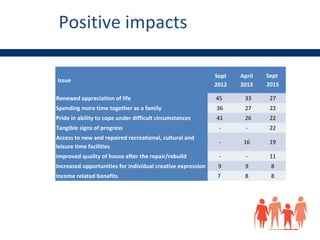



The document discusses the social and psychosocial impacts of earthquakes on recovery in Canterbury, New Zealand, highlighting various surveys that measure quality of life and stressors. It notes prevalent negative impacts like dealing with insurance issues and being in a damaged environment, alongside positive impacts such as renewed appreciation for life. Additionally, it emphasizes the need to learn from past disasters and addresses the mental health impacts on vulnerable populations.

![PreventionWorks2009-10[1]](https://cdn.slidesharecdn.com/ss_thumbnails/6e295157-6c8c-460e-b123-021629d05455-150422001250-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)

















































































