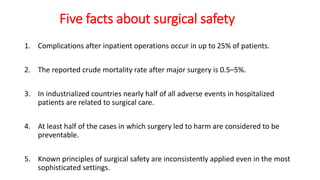
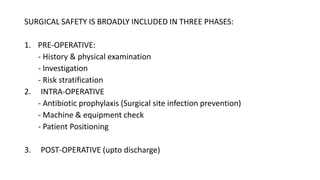
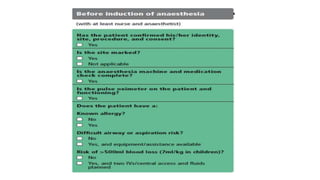
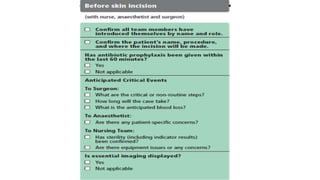
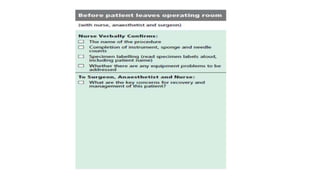
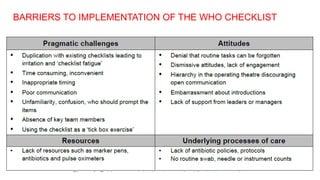
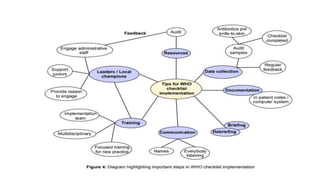
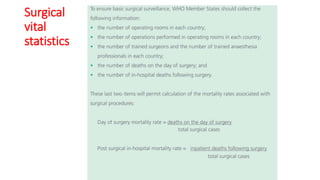
The document discusses principles of safe surgery and outlines three phases of surgical safety: pre-operative, intra-operative, and post-operative. It notes that complications occur in up to 25% of patients after surgery and half of adverse surgical events are considered preventable. The World Health Organization introduced a surgical safety checklist to encourage safety checks and minimize preventable patient harm during procedures. Barriers to fully implementing safety standards include inconsistent application of principles and checklists across healthcare settings.