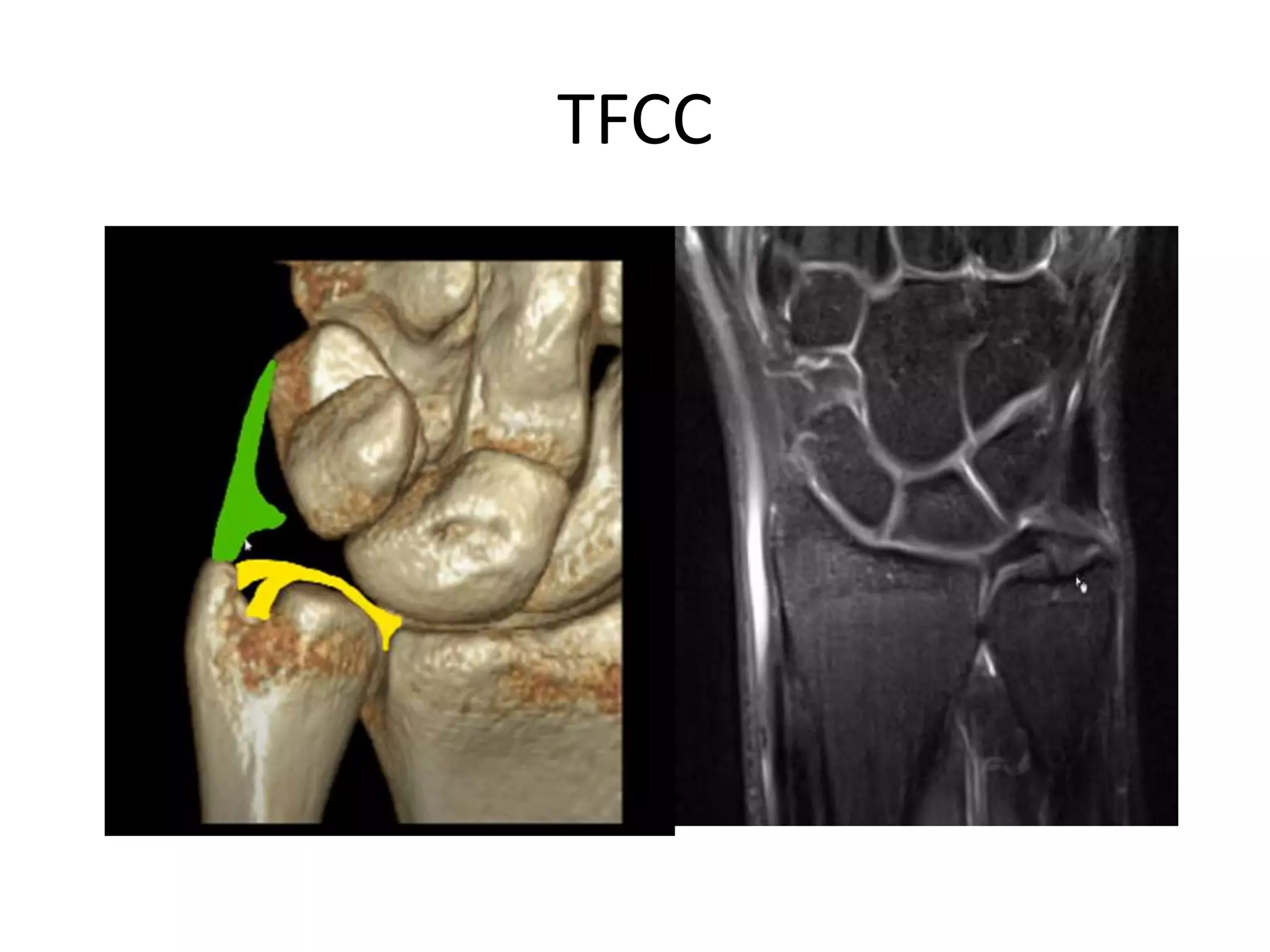
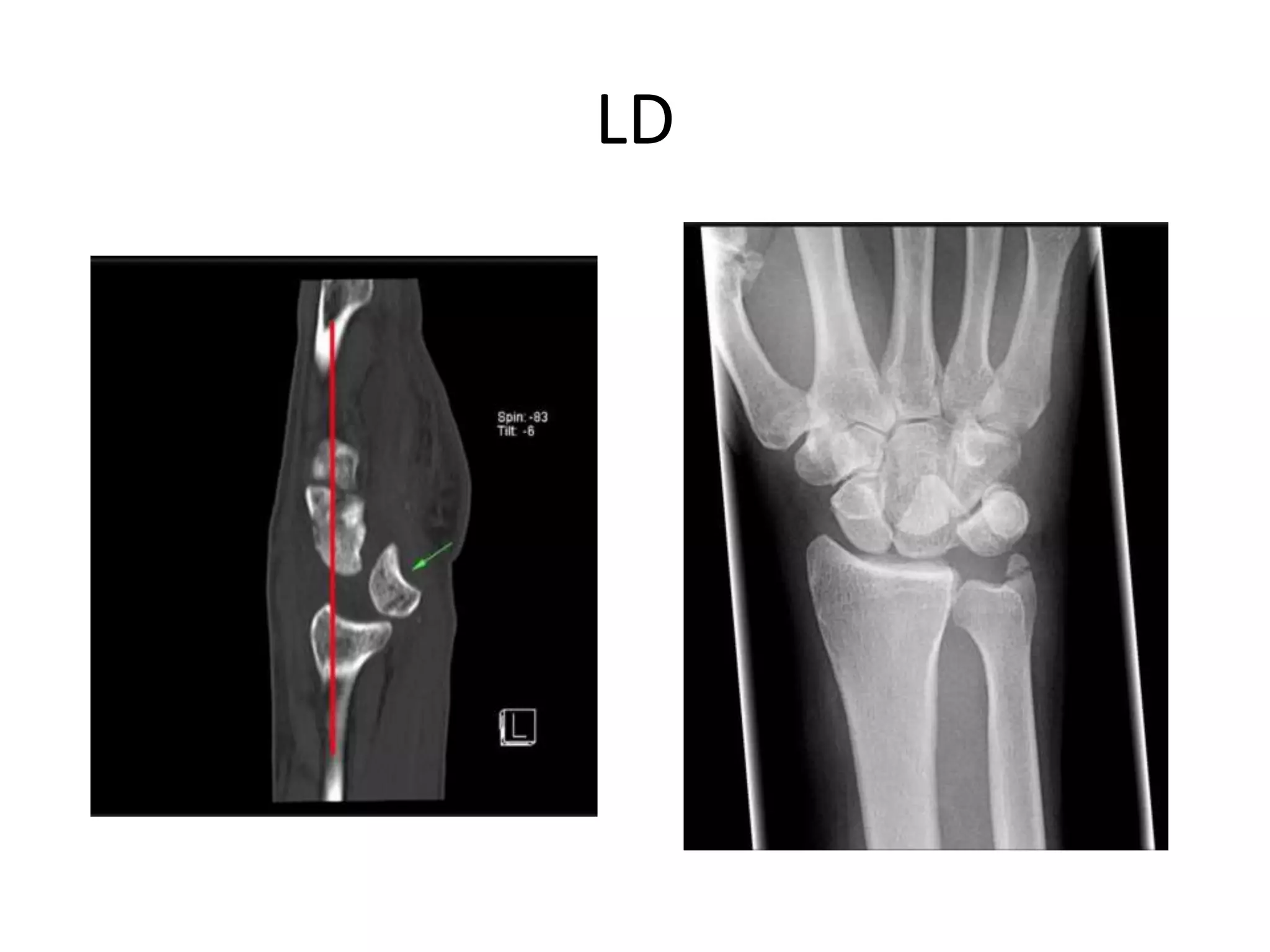
This document provides an overview of imaging of the wrist joint. It begins with an introduction to the anatomy of the wrist joint and the role of x-ray and MRI in evaluation. Specific anatomical structures are then described such as the carpal arcs, axes, angles, ligaments and neurovascular structures. Common pathologies are discussed including tears of the triangular fibrocartilage complex (TFCC), scapholunate dissociation, lunate dislocations, and Kienbock's disease. Imaging appearances of these conditions on x-ray, ultrasound and MRI are presented. Other topics covered include ulnar variance, carpal tunnel syndrome, Guyon's canal syndrome, and intersection syndromes.