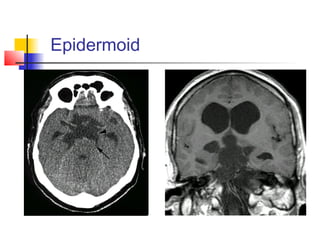
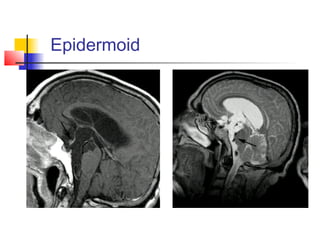
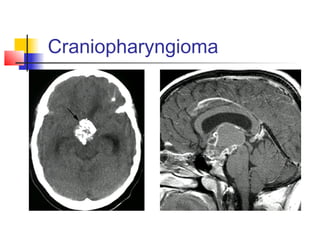
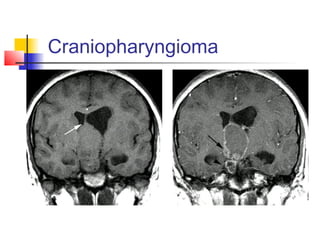
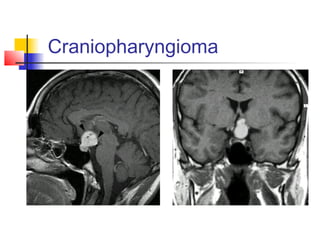
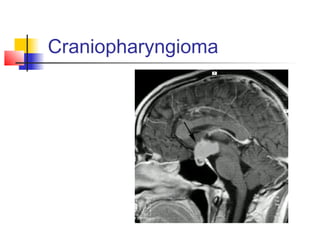
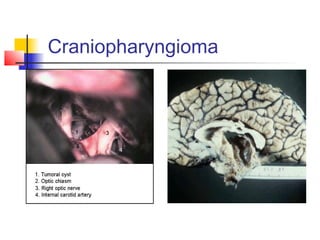
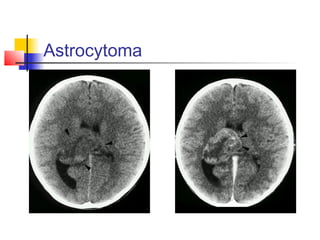
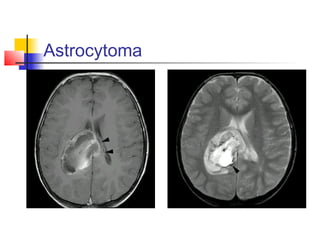
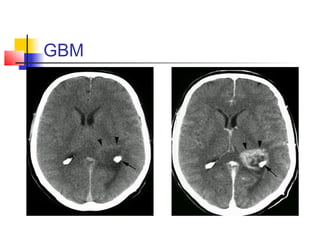
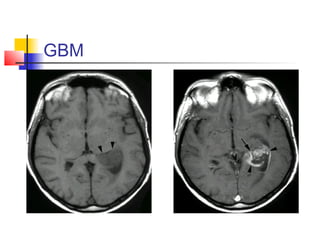
The document discusses various masses that can occur in the third and lateral ventricles. It describes 10 types of anterior third ventricular masses including astrocytomas, ependymomas, germinomas, metastatic tumors, epidermoid tumors, craniopharyngiomas, colloid cysts, pituitary tumors, and others. It also describes 7 types of posterior third ventricular masses and 8 types of lateral ventricle masses. For each mass, it provides information on symptoms, imaging appearance, diagnosis, and treatment options.