RADIOLOGICAL IMAGING OF COLITIS
•Download as PPTX, PDF•
17 likes•4,925 views

Health &medicine.

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to RADIOLOGICAL IMAGING OF COLITIS
Similar to RADIOLOGICAL IMAGING OF COLITIS (20)
More from Abdellah Nazeer
More from Abdellah Nazeer (20)
Recently uploaded
Recently uploaded (20)
RADIOLOGICAL IMAGING OF COLITIS
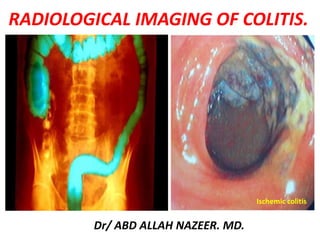
- 1. RADIOLOGICAL IMAGING OF COLITIS. Dr/ ABD ALLAH NAZEER. MD. Ischemic colitis
- 2. TYPES OF COLITIS: • IBD: UC and Crohn’s. • Infectious colitis. • Ischemic colitis. • Diverticulitis (DDX: EA). • Neutropenic colitis. • Drug-related colitis.
- 3. FEATURES OF COLITIS: Nonspecific signs: • Wall thickening. • Target sign. • Hyperemia (comb sign). • Pericolonic stranding. • Ascites.
- 4. FEATURES OF COLITIS: Specific signs: • Distribution • Lymph nodes. • Fistulae • Sinus tract. Distribution: • Right, left or diffuse • Skip areas • Rectum spared • Focal only
- 5. DISTRIBUTION: IBD & INFECTIOUS COLITIS: Ulcerative Colitis. CMV (or right). E. coli. PMC (or left). Campylobacter. Crohn's. Diffuse in Colon Right Colon(+TI) Left Colon Crohn’s. TB. Yersinia. Salmonellosis. Amebiasis. (Typhlitis). Ulcerative Colitis. Shigellosis. Schistosomiasis. Herpes. Lymphogranuloma. (Drug -induced col.).
- 6. Segment Thickness Extension Small Bowel Rectum Halo Sign Ischemia G>D 8-10 Long + - + Crohn's D>G 10-15 Long +++ + +++ Ulcerative Colitis G 6-8 Long - +++ +++ Infectious Colitis D>G 8-10 Long ++ + +++ Pseudo- Membranous Colitis G>D 10-15 Long - - +++ ETIOLOGIC DIAGNOSIS:
- 9. Degree of mural thickening.
- 11. Crohn's disease is an idiopathic inflammatory bowel disease (IBD) characterized by widespread gastrointestinal tract involvement typically with skip lesions. It is also known as regional enteritis, and frequently there is systemic involvement. Radiographic Features: Fluoroscopy Features on barium small bowel follow-through include: mucosal ulcers aphthous ulcers initially deep ulcers (more than 3mm depth) longitudinal fissures transverse stripes when severe leads to cobblestone appearance may lead to sinus tracts and fistulae widely separated loops of bowel due to fibro-fatty proliferation (creeping fat) thickened folds due to edema Pseudo-diverticula formation: due to contraction at the site of ulcer with ballooning of the opposite site string sign: tubular narrowing due to spasm or stricture depending on chronicity partial obstruction on control films presence of gall stones, renal oxalate stones, and sacroiliac joint or lumbosacral spine changes should be sought.
- 12. CT examination can be carried out with both intravenous and intraluminal contrast (positive or negative): fat halo sign comb sign bowel wall enhancement bowel wall thickening (1-2 cm) which is most frequently seen in the terminal ileum (present in up to 83% of patients). strictures and fistulae mesenteric/intra-abdominal abscess or phlegmon formation abscesses are eventually seen in 15-20% of patients MRI enterography (MRE) MR enterography can be a useful technique for evaluation of the bowel. Inflamed loops of bowel demonstrate thickening and contrast enhancement. Extramural disease is where MRI excels: fibrofatty proliferation: thickening of extramural fat, which separates bowel loops equivalent to the fat halo sign on CT vascular engorgement: comb sign stenosis and strictures.
- 13. Crohn's Disease – Barium Images.
- 15. CROHN’S DISEASE: SMALL BOWEL.
- 17. CT and MR Enterography for Crohn's Disease.
- 18. Crohn's disease. Coronal fluid sensitive (T2), T2 fat suppressed and T1 post contrast images. Red arrows outline the diseased colon with wall thickening, abnormal edema and ascites (thin arrow) and intense post contrast enhancement. Yellow arrows highlight proliferation of mesenteric vessels in creeping fat, commonly referred to as the “comb” sign.
- 20. Ulcerative colitis is an inflammatory bowel disease that not only predominantly affects the colon, but also has extraintestinal manifestations. Radiographic features Involvement of the rectum is almost always present (95%), with the disease involving variable amounts of the most proximal colon, in continuity. The entire colon may be involved, in which case edema of the terminal ileum may also be present (so-called backwash ileitis). Plain radiograph Non-specific findings, but may show evidence of mural thickening (more common), with thumbprinting also seen in more severe cases. Fluoroscopy Mucosal inflammation leads a granular appearance to the surface of the bowel. As inflammation increases, the bowel wall and haustra thickened. Mucosal ulcers are undermined (button-shaped ulcers). When most of the mucosa has been lost, islands of mucosa remain giving it a pseudopolyp appearance. In chronic cases, the bowel becomes featureless with the loss of normal haustral markings, luminal narrowing and bowel shortening (lead pipe sign). Small islands of residual mucosa can grow into thin worm-like structures (so- called filiform polyps) Colorectal carcinoma in the setting of ulcerative colitis is more frequently sessile and may appear to be a simple stricture.
- 21. CT: CT will reflect the same changes that are seen with a barium enema, with the additional advantage of being able to directly visualise the colonic wall, the terminal ileum and identify extra-colonic complications, such as perforation or abscess formation. It is important to note however that CT is insensitive to early mucosal disease. In chronic cases, fat submucosal deposition is seen particularly in the rectum (fat halo sign). Also in this region, extramural deposition of fat, leads to thickening of the perirectal fat, and widening of the presacral space . Strictures are also common and are not all malignant. These are predominantly due to marked muscularis mucosa hypertrophy, which is also in part responsible for the lead pipe sign. MRI: The most striking abnormalities in ulcerative colitis are wall thickening and increased enhancement. The median wall thickness in ulcerative colitis ranges from 4.7 to 9.8 mm. In general, the more severe the inflammation, the thicker the colonic wall. A colonic wall thickness <3 mm is usually considered as normal, 3-4 mm as a "gray zone," and >4 mm as pathological. Enhancement of the mucosa with no or less enhancement of the submucosa producing a low SI stripe—the so-called submucosal stripe.
- 23. Ulcerative colitis with lead pipe appearance.
- 26. MRI Images with ulcerative colitis.
- 27. MRI Images with ulcerative colitis.
- 29. Cytomegalovirus (CMV) is a member of the Herpes viridae family, along with herpes simplex viruses 1 and 2, Epstein-Barr virus, and varicella-zoster virus. It is a double-stranded DNA virus with a protein coat and lipoprotein envelope. Similar to other herpes viruses, CMV is icosahedral and replicates in the host's nucleus. Replication in the host cell typically manifests pathologically with large intra-nuclear inclusion bodies and smaller cytoplasmic inclusions, and is accompanied by the presence of CMV viral particles in the plasma. Radiographic features Barium studies CMV oesophagitis Small well-circumscribed ulcers are present, with the mucosa between them appearing normal. Larger (~2cm) superficial mid-esophageal ulcers are said to be relatively characteristic of CMV oesophagitis . Deep ulceration is uncommon. CMV gastritis Typically the antrum is involved, and it has a nodular mucosal pattern with luminal narrowing. CT CT is particularly useful in CMV enterocolitis. The appearances are similar to that of inflammatory bowel disease, with mural thickening and surrounding stranding, although often the thickening is patchy and not circumferential. Ascites is seen in almost half of cases. Both diffuse and segmental involvement is encountered . In some instances the appearances are essential normal and biopsy is therefore still required when clinical symptoms are suspicious. Involvement of the small bowel is less frequent, seen in only 42% of cases. Lymph node enlargement is usually not present. Perforation has the usual imaging hallmarks of free intraperitoneal fluid and gas.
- 31. CMV ileocolitis in a 30 years old patient with aids: important wall thickening related to submucosal edema CMV inclusions showed are shown at biopsy.
- 32. Circumferential ulcerated stricture. Markedly thickened folds of the transverse and descending colon, consistent with pseudo- membrane formation.
- 33. INFECTIOUS COLITIS: •Diagnosis: clinical aspects suggesting some infections (tuberculosis, amoeba, CMV) •Confirmed by specific lab tests + colonoscopy and biopsy •CT features: –Right colon + ileum = salmonella, amoeba, tuberculosis,, yersinia –Left colon = schistosoma, shigella, herpes, syphilis –Pan colonic : CMV, E Coli •Tuberculosis: (may mimic Crohn's disease) –Clinical context –Caecum granuloma with necrosis on biopsy –Ileocæcal location –Transmural injury –Wall thickening –Enlarged lymph nodes with low attenuation –Ascites –Fistulae/abscess •Amebiasis: –Endemic countries –Differential diagnosis : appendicitis –Diffuse ulcerations at biopsy, with presence of the parasite –Acute fulminant colitis –Ìleocaecal is the preferred location but the entire colon can be involved –Liver abscesses help in the positive diagnosis.
- 34. Tuberculosis colitis in a 25 years old patient : wall thickening of the caecum , enlarged lymph nodes with low attenuated center and ascites are seen.
- 37. Amoeba colitis of the Caecum in a 40 years old patient : liver abscesses are seen.
- 39. Right -sided colitis in a patient with cirrhosis and portal hypertension. The endoscopic images are of different patient with right-sided colitis.
- 40. •Pseudomembranous colitis: - Mean age: 50 years –Diarrhea –Abdominal pain –Fever, anorexia, nausea, dehydration •Recent use of antibiotics or recent surgery •Clostridium difficile, toxins in the stools •Colonoscopy: –Ulcerations, creamy, white and elevated plaques or nodules, volcano like eruptions of fibrin and leukocyte from mucosal crypt •Entire colon+++ involvement •Small bowel can be involved •Important wall thickening (mean :11mm) •Accordion sign, nodular/polypoid = submucosal edema •Thumbprinting •Pericolonic fat stranding •Ascites
- 41. Pseudomembranous colitis in a 34 years old patient with recent use of antibiotics: follow up J4, aspecific colonic wall thickening.
- 42. Pseudomembranous colitis. (Left) Axial CT scan of the mid-abdomen utilizing oral but not intravenous contrast demonstrates marked thickening of the colonic wall (white arrows) producing the so-called "accordion sign." There is a small amount of pericolonic stranding (red arrow) and ascites (green arrow). (Right) Axial CT scan through the pelvis shows marked thickening of the wall of the rectum (yellow arrows) indicating this is a pan-colitis.
- 43. Pseudomembranous Colitis with dilatation of the sigmoid. Pseudomembranous Colitis.
- 46. DRUG INDUCED COLITIS: •Chemotherapy (mucosal ulcerations, inflammation) •Antibiotics (clostridium difficile) •Vasoconstrictors, drug for hypertension, oral contraceptives (ischemia, inflammation) NSAID
- 47. Toxic colitis involving the entire colon in a 40 years old patient, 48H after the colonoscopy.
- 48. NEUTROPENIC COLITIS: •Clinical aspects: –Immunodepression : leukemia, HIV, transplantation, chemotherapy –Bacteria, viruses, and fungi grow profusely in the absence of neutrophils •Lab tests : Immunodepression, non specific •Colonoscopy: –Same features than ulcerative colitis or infectious colitis, but only the right colon is involved –Hyperemia, edema, and superficial ulcerations •Ìleocaecal, and right colon involvement •Important circumferential wall thickening (up to 3 cm for the caecum, 4mm for ileum) •Parietal low attenuation, submucosal edema •Parietal pneumatosis (severity sign) •Pericolonic stranding •Sepsis, abscess, intestinal necrosis, hemorrhage may occur
- 49. Neutropenic colitis involving the entire colon and ileum in a 30 years old patient : ascites, circumferential wall thickening are shown.
- 50. Neutropenic colitis. Computed tomography (CT) in an 18-year-old man with acute myelogenous leukemia, fever, and neutropenia. A, Axial CT image shows the marked thickening of the caecum and a small amount of free fluid. B, Coronal CT reformat shows pancolitis, affecting the right colon to a greater extent.
- 51. Typhlitis in a patient with neutropenia.
- 52. Radiation induced colitis in a 70 years old woman with radiation exposure : left colon wall thickening, stricture of is caliber are shown
- 53. Diverticulitis is one of the presentations of diverticular disease and is most often a complication of colonic diverticulosis. Differentiating one from the other is critical since uncomplicated diverticulosis is mostly asymptomatic and acute diverticulitis is a potentially life-threatening illness. Radiographic features CT is the modality of choice for the diagnosis and staging of diverticulitis. Appearances include: pericolic stranding, often disproportionately prominent compared to the amount of bowel wall thickening segmental thickening of the bowel wall enhancement of the colonic wall usually has inner and outer high-attenuation layers, with a thick middle layer of low attenuation diverticular perforation extravasation of air and fluid into the pelvis and peritoneal cavity abscess formation (seen in up to 30% of cases) may contain fluid, gas or both fistula formation gas in the bladder direct visualization of a fistulous tract
- 55. Sigmoid diverticulitis with abscess formation: sigmoid colon displaying mural thickening, diverticulosis and pericolic fat stranding (arrow). Adjacent low attenuation, septated collection (circle) representing abscess formation, with adhesion noted to adjacent small bowel loops.
- 56. Perforated sigmoid diverticulitis: sigmoid colon displaying diverticulosis, mural thickening and pericolic inflammatory fat stranding (arrow) with adjacent collection of intra-abdominal free air and adjacent inflammatory fat stranding (circle), again representative of active diverticulitis with perforation.
- 58. Ischemic colitis refers to inflammation of the colon secondary to vascular insufficiency and ischemia. It sometimes considered under the same spectrum of intestinal ischemia. The severity and consequences of the disease are highly variable. Epidemiology Ischemic bowel is typically a disease of the elderly (age >60 years) where atherosclerotic disease or low flow states are usually the cause 2. In younger individuals, the disease is more likely to be related to vasculitis or hyper coagulable states. The causes can be categorized as follows: arterial occlusion: arteriosclerosis vasculitides arterial emboli venous thrombosis: hyper coagulative states including malignancy and OCP use primary mesenteric venous thrombosis low flow states: hypotension congestive heart failure cardiac arrhythmias others: sickle cell disease radiation therapy
- 59. Radiographic features Plain film: abdominal radiograph Abdominal radiographs are often normal, but signs include: dilatation due to ileus 'thumbprinting' due to mucosal edema/hemorrhage localized intramural gas (pneumatosis coli) if necrotic free intraperitoneal gas if perforated Fluoroscopy: barium studies Contrast enema is abnormal in 90% but is rarely used for diagnostic purposes: segmental region of abnormality 'thumbprinting' which is classically obliterated by air insufflation. spasm ulcerations 'serated mucosa’ stricture from fibrosis as a late complication of ischemia CT Contrast enhanced imaging is the modality of choice. Features include: segmental region of abnormality symmetrical or lobulated thickening of bowel wall irregularly narrowed lumen Submucosal edema may produce low-density ring bordering lumen (target sign) intramural or portal venous gas Mesenteric edema superior mesenteric artery or vein thrombus/occlusion may be demonstrated.
- 60. Angiography Can show mesenteric artery occlusion if present. Otherwise, angiography may show increased arterial caliber, accelerated arteriovenous transit time and dilated draining veins due to the inflammatory response. In mesenteric venous thrombosis, the veins may not be visualized, and collateral venous filling may be seen. Ultrasound Ultrasound is of limited use due to bowel gas but may show: luminal thickening over the affected segment with or without stratification hypoechoic wall due to edema areas of increased echogenicity if hemorrhage echogenic foci with shadowing if intramural gas reduced peristalsis may be observed Doppler imaging of the SMA origin can be useful in assessing for stenosis Nuclear medicine Increased uptake of Tc99m (V) DMSA tracer in the ischaemic bowel may be present but is unreliable
- 62. Ischemic colitis: parietal pneumatosis is seen on the right side of the scout view Ischemic colitis, CT: coronal view showing wall thickening with pericolonic fat stranding
- 63. CT Images for Ischemic colitis.
- 64. CT Images for Ischemic colitis.
- 65. CT Images for Ischemic colitis.
- 66. CT Images for Ischemic colitis.
- 67. Magnetic resonance imaging follow-up of a patients with ischemic colitis resolved promptly. Ischemic colitis (IC) of left side colon in a 57 year old woman with a recent history of acute hypertensive crisis, who presented with left lower quadrant pain and massive rectal bleeding. A: Endoscopic procedure showed multiple necrotic area; B and C: Contrast-enhanced computed tomography (CT) and axial T2 fast-recovery fast-spin echo sequence (FRFSE) magnetic resonance imaging (MRI), after 32 h from CT, showed acute IC (Type I CT and MRI) with wall thickening, three layer sandwich sign and a mild amount of free fluid in the parabolic gutter; D and E: 2D coronal reformat CT and coronal T2 FRFSE MRI, at the same time, showed the entire involved tract; F: Ischemia resolved without complications with conservative therapy as shown in the follow-up MRI.
- 68. Magnetic resonance imaging follow-up of a patient with ischemic colitis and worsening of clinical symptoms. Ischemic colitis (IC) of sigmoid colon in a 62-year-old man with left lower quadrant pain and elevate lactate dehydrogenase levels, who presented with melena and a recent history of stenting procedures for ischemic cardiopathy. A: Endoscopic procedure showed multiple necrotic area; B: 2D (two dimensional) coronal reformat contrast-enhanced computed tomography (CT) showed acute IC (Type I CT); C-E: The patient had 2 magnetic resonance examinations (C and D-E) with an interval of 48 h due to worsening of clinical symptoms, with an increase of the length and thickness of the involved tract (D-E); F: The ischemic process resolved without complication after parenteral nutrition, as showed in the follow-up magnetic resonance imaging, performed after 384 h from the date of CT examination.
- 69. 7T magnetic resonance imaging investigation. A: Image of a 7T magnetic resonance imaging (MRI) abdominal scan before inferior mesenteric artery (IMA) ligation; B: A 7T MRI abdominal scan 1 h after IMA ligation; C: At 4 h after IMA ligation; D: At 6 h after IMA ligation; E: At 8 h after IMA ligation; F: Image of 7T MRI colon enema.
- 70. Thank You.