Presentation1, Ultrasound of the bowel loops and the lymph nodes..pptx
•Download as PPTX, PDF•
1 like•269 views

Ultrasound of the bowel loops and the lymph nodes..pptx

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Presentation1, Ultrasound of the bowel loops and the lymph nodes..pptx
Similar to Presentation1, Ultrasound of the bowel loops and the lymph nodes..pptx (20)
More from Abdellah Nazeer
More from Abdellah Nazeer (20)
Recently uploaded
Recently uploaded (20)
Presentation1, Ultrasound of the bowel loops and the lymph nodes..pptx
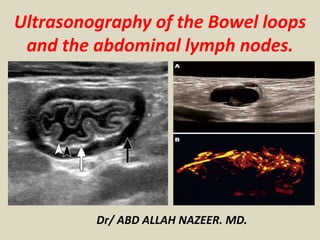
- 1. Ultrasonography of the Bowel loops and the abdominal lymph nodes. Dr/ ABD ALLAH NAZEER. MD.
- 2. Normal bowl wall anatomy: The bowl wall consists of 5 layers, of different echogenicity. Typically, only 2 layers are visible on US, including an inner hyperechoic layer and outer hypoechoic layer. Normally, bowel loops are compressible, show minimal vascularity, and have wall thickness < 2 mm. Technique: It is mandatory to check the SMA/SMV relation in every case Scan is started with a 3.5- to 8-MHz convex probe to provide a broad overview, to assess the extent of bowel involvement and to avoid overlooking of extra-intestinal “deeper” associated findings. Then a high-frequency (4–13 MHz) linear array probe is used to assess bowel wall thickness and wall layer discrimination. Specific technique tips and tricks will be discussed in detail at each pathology.
- 3. Normal “gut signature” Mucosal interface with lumen (hyperechoic), mucosa (hypoechoic), submucosa (hyperechoic), muscularis propria(hypoechoic) and serosa (hyperechoic). B: Normal SMA/SMV relationship in gray scale and color Doppler image.SMA has echogenic rim and seen to the left of the SMV.
- 4. Normal gastrointestinal tract in ultrasound. A:Normal pylorus. B: Normal duodenum. C: Normal proximal jejunal loops in LUQ. D:Normal ileal loops in the right lower quadrant. E: Normal appendix. F: Normal colon (orange arrows-Haustra).G:Normal distal jejunal loops in the LLQ.
- 5. Pathologies: Hypertrophic Pyloric Stenosis (HPS) vs. pyloric spasm: Ultrasound technique: The baby is placed in the right oblique position, first the gallbladder is identified, as the pylorus is usually located slightly medial and posterior to the gallbladder, then assess the appearance and measurements of the pylorus. Finally, assess the gastric emptying through the pylorus and the presence of hyperperistalsis. If the stomach is empty, the baby is fed with small amount of water. HPS is common in males (M: F= 4:1), diagnosed in those aged 3-12 weeks. Babies present with projectile non-bilious vomiting, due to thickened pyloric muscularis propria. In pyloric spasm, the muscularis propria is either not hypertrophied, or slightly thick, but < 3 mm thick, with visualized pyloric opening. Pyloric spasm requires observation while HPS is treated with surgical pyloromyotomy.
- 6. 6 week old baby with projectile vomiting for 1 week. Target sign/doughnut sign/ CERVIX sign, with symmetrical muscular wall thickening of 5 mm, elongated pyloric canal (20 mm) Double internal layer of crowded mucosa (nipple sign "arrow") Lack of gastric emptying with hyperperistalsis; typical of hypertrophic pyloric stenosis. B: The pyloric canal is 10 mm long and muscularis propria is 3 mm in thickness, mild gastric emptying, ongoing with pyloric spasm. C: examination in the right oblique position, using linear transducer parallel to the right costal margin.
- 7. Intramural Duodenal hematoma: Ultrasound technique: The epigastric region is surveyed with a linear transducer, duodenal hematoma is seen lateral or posterior to the pancreatic head. It may occur as a result of blunt abdominal trauma, non-accidental injury to children. The retroperitoneal attachment and the lack of a mesentery along with the proximity of especially the third part to the spine may account for vulnerability in blunt
- 8. 2 year old with vomiting and history of trauma 3 days ago. A:a heterogenous, hypoechoic with irregular cystic areas, well defined lesion in the epigastric region, B: no internal vascularity demonstrated on color Doppler. CT was done to confirm the diagnosis of duodenal hematoma. C & D: Axial with (E) coronal enhanced CT images of the upper abdomen, show cystic non enhancing lesion in the location of the 2nd and 3rd parts of the duodenum (H).
- 9. Midgut volvulus: Ultrasound technique: The position of superior mesenteric artery (SMA) in relation to superior mesenteric vein (SMV) is recorded in gray scale and Color Doppler imaging. Whirlpool sign is looked for and finally the peristalsis, diameter, vascularity and collapsibility of the rest of the bowel loops is assessed. Inverse orientation of the superior mesenteric artery (SMA) and the superior mesenteric vein (SMV) (i.e. SMV seen to the left or SMA) is a sign of malrotation. Whirlpool sign, corresponding to a clockwise wrapping of the SMV around the SMA, has a high predicting value and is an imaging characteristic of midgut volvulus.
- 10. 7-month-old boy. abnormal SMA/SMV correlation was seen, Color Doppler ultrasound in the epigastric region show whirling vessels and was diagnosed with mid gut volvulus.
- 11. Incarcerated/ Strangulated inguinal hernia: Ultrasound technique: Both inguinal regions along with scrotum are examined with linear transducer, presence of bowel peristalsis, wall thickness and vascularity are recorded. The bowel, ovaries, or fallopian tubes are the organs that most commonly incarcerate into the inguinal region, through a patent processus vaginalis, which may progress rapidly to strangulation (vascular compromise and infarction) of the incarcerated contents. (Fig.6)
- 12. An 8 month old boy with scrotal swelling and abdominal distension. Longitudinal images through the inguinal region, show dilated, thick hyperechoic walled, fluid filled, aperistaltic small bowel loop seen superior to the testis (*) with preserved vascularity. Findings are consistent with incarcerated inguino-scrotal hernia.
- 13. Henoch Schönlein Purpura HSP is a small-vessel, immune-mediated vasculitis associated with immunoglobulin A (IgA) deposition. Peak incidence 3-10 years. Gastrointestinal symptoms are encountered in 70% of the cases. Seen as multifocal bowel thickening, vascular engorgement and intussusception, typically ileoileal type.
- 14. 8 year old boy, known case of Henoch Schonlein Purpura, (1)long segment of thickened ileal bowel loop in the right lumbar region, (2) in the right iliac fossa and (3) a short segment of thickened jejunal loop in the left upper quadrant, with normal peristalsis. All thickened bowel loops are fluid filled,loss of normal stratification, due to intramural hemorrhage.
- 15. Crohn’s disease: Crohn's disease may present with acute, appendicitis-like symptoms. US may play an important role in establishing the initial diagnosis, assessing the extent of bowel involvement and diagnosing possible complications. The sensitivity of US for detecting ileocecal Crohn's disease of over 95%.
- 16. Axial US images of a 12 year old girl, a known case of crohn’s disease in remission. (A): Hypoechoic thickened terminal ileal wall with total loss of stratification, fatty aggregation (B) mild hypervascularization at color-Doppler. (C)Thickened colon in the right lumbar region. (D&E) follow up study done 6 months post treatment, shows mild ileal and colonic thickening with preserved stratification and significant regression of fatty aggregation.
- 17. 14year old boy, with abdominal pain and vomiting. Irregularly thickened long segment of ilium extends from RIF (A) till the supra-pubic region (B&C) with loss of normal stratification and significant surrounding fatty aggregation (*) a sign of longstanding Crohn’s disease. Axial balanced FFE (D) and post contrast T1 MR images of the correspond to the US findings
- 18. 14 year old boy, known case of Crohn’s disease, (A) axial enhanced CT image of the lower abdomen show thickened segments of ileal bowel loops and ascending colon, mucosal enhancement, surrounding free fluid and fat stranding in going with active Crohn’s disease. He presented with vomiting and high inflammatory markers 6 months after initial diagnosis (C) US of the pelvis shows a large collection with multiple air foci, confirmed by CT (D & E).
- 19. Idiopathic Ileocolic vs. Eneteroenteric Intussusception: Ultrasound Technique: Bowel is screened with five to six vertically oriented, overlapping lanes 'mowing the lawn technique' using a linear high frequency probe. Intussusception occurs when a proximal bowel loop invaginate into an adjacent distal bowel loop, typically within the ileocecal region, 90% of the time without a lead point, rather due to hypertrophy of Peyer’s patches. Predominantly seen in children 3 months to 3 years of age. When it occurs outside of the typical age range, it is likely to be associated with a pathologic lead point (Meckel’s diverticulum, duplication cyst, polyps, non-Hodgkin’s lymphoma). Small bowel intussusception is transitory, usually seen in the side of the abdomen during scanning. It contains less mesenteric fat and lymph nodes, with a small outer diameter (less than 2.5 cm), short segmental invagination (less than 3 cm), and peristaltic wall motion.
- 20. Baby girl, with vomiting and colic. (A) Concentric parallel rings of bowel wall ”Target/ doughnut or pseudokidney sign” ,in the RUQ, its diameter >2.5 cm, ongoing with ileocolic intussusception. (B) Color Doppler: preserved vascularity. (C) longitudinal view: long segment of invagination (opposed to short segments seen in enteroenteric intussusception. (D) Another case with ileocecal intussusception, notice layering of fluid between the telescoped bowel loops and mesenteric lymph nodes, when seen reflects decreased probability of reducability. (E) A case of entero-enteric intussusception seen in the LUQ, its diameter <2.5 cm. Self limited, needs no reduction.
- 21. Acute Appendicitis: Ultrasound Technique: Graded-compression is applied with the linear transducer at the point of maximal tenderness. If no abnormality is seen, a thorough search for direct or indirect signs of appendicitis in the right iliac fossa, right lumbar and subhepatic regions is sought[6] in supine and left oblique positions. Most commonly occurs in school agers. Diagnosis can be challenging as inflammatory markers are not elevated in 20% of cases and clinical presentation is variable or atypical in 30-45% of cases, especially in the preschool agers.
- 22. Atypical locations of the appendix.
- 23. Direct and secondary signs of acute appendicitis as reported by Gerhard Mostbeck et al, ‘’ How to diagnose acute appendicitis:
- 24. 7 months baby, with vomiting and bloody diarrhea, a case of phlegmonous acute appendicitis. US of the right hypochondrial region show thickened non compressible appendix, with preserved stratification, omental fatty aggregation (*) and an overlying dilated hyperechoic small bowel loop (B). B: 8 year old, a case of gangrenous acute appendicitis. The appendix shows interruption of the mucosal continuity (->),hypervascularity and periappendiceal fatty prominence (*).
- 25. A 2 year old boy, with abdominal pain for 3 days and vomiting. Acute gangrenous tip appendicitis with interrupted mucosa (->), appendicolith (A) and fatty aggregation superior to the inflamed tip, peri-ileal (*) The normal proximal appendix (N)
- 26. (A): A 4 year old, x-ray shows dilated small bowel loops. US shows fluid filled dilated bowel loops in the LLQ with hyperechoic thickened wall and hypoperistalsis. RIF has ill- defined hypoechoic fluid (F) and omental fat (*) prominence, suggestive of perforated appendix. (B) Another case of perforated appendicitis, characterized by disruption of the entire thickness of the appendicular wall with periappendiceal free fluid.
- 27. 4 different cases of appendicular abscesses (A&B) are subhepatic,(C,D&E) are pelvic, showing varying echogenicities, ranging from cystic with internal debris (A), hypoechoic (B), heterogenous predominantly hypoechoic (C), heterogenous with predominant cystic component (D) or heterogenous with an appendicolith.
- 28. Algorithm for acute appendicitis diagnosis.
- 29. Acute gastroenteritis Symptom-wise, the commonest mimicker of acute appendicitis. the most common causes of gastroenteritis in children are viruses (rotaviruses, adenoviruses, enteroviruses), bacteria (food poisoning, pathogens like Salmonella, E. Coli, Listeria), and intestinal parasites (like amoeba histolytica & Giardia lamblia).
- 30. A 3-year-old girl, with vomiting and bloody diarrhea. Thickened sigmoid colon seen with predominant submucosal layer thickening. (B & C)diffusely thickened colon in the RIF/LIF, with loss of Normal bowel stratification. Small bowel loops were not thickened.
- 31. TUS in Celiac Disease Despite the fact, that gold standard for the diagnosis of celiac disease is histologic confirmation of the intestinal damage in serologically positive individuals, in patients with untreated celiac disease we can regularly find out several sonographic signs that raise suspicion of this chronic disease also in clinically asymptomatic persons. Increased fluid content in moderately dilated bowel loops (25 to 35 mm) with hyperperistalsis in fasting state, lightly thickened bowel wall (3–5 mm) and thickened valvulae conniventes are most frequently seen in patients with untreated celiac sprue. Reduced number of jejunal folds and increase of ileal folds (jejunalization of ileum) intermittent intussusceptions due to hyperperistalsis, presence of slightly enlarged mesenterial lymph nodes (5–10 mm in short axis)and dilatation of SMA with low resistive index are also very frequent. In comparison to controls, celiac patients had higher superior mesenteric artery blood velocity and flow, with lower resistance indexes and higher portal vein velocity and flow in comparison to controls. Presence of small amount of free peritoneal fluid and increased gallbladder volume are also seen in these patients.
- 32. Celiac sprue: (a) Dilated loops of small bowel with thickened wall, and valvulae conniventes hyperperistalsis— standard abdominal probe. (b) Intussusception of jejunum in transverse (left) and longitudinal section in celiac sprue—high resolution probe. (c) Dilated SMA (9 mm) in a patient with untreated celiac disease—standard probe. (d) Low resistive index-RI (0.69) in SMA in untreated celiac disease—standard probe.
- 33. Acute pancreatitis: It is rare in children, occurs in all age groups. Diffuse or focal enlargement of the pancreas is attributable to edema; however, pancreatic enlargement has been reported to be absent on ultrasound in approximately 50% of the patients.
- 34. A 30 month old girl, with vomiting. Ultrasound showed (A) hyperechoic pancreatic parenchyma (B) Bulky pancreatic head (H) with fluid in the lesser sac (open arrow), C: Rim of hypoechoic peri-pancreatic fluid (arrow) and heterogeneous body - tail junction (*) D: companion case of normal pancreas, iso-echoic to the liver.
- 35. Etiology of acute pancreatitis in children
- 36. Focal acute bacterial nephritis: It is due to a localized non- liquefactive inflammatory renal bacterial infection and considered to be a midpoint in the spectrum ranging from uncomplicated pyelonephritis to intrarenal abscess.
- 37. 8 year old boy, with fever and vomiting. (A) A geographic area of hypoechogenicity in the upper pole of the right kidney (*), (B) Color Doppler image shows patent renal vein and segmental renal arteries, (C ) Power Doppler image shows focal hypoperfusion of the upper polar renal parenchyma (*), (D) Coronal enhanced CT image shows right upper polar wedge shaped enhancement defect (arrow) no abscess formation.
- 38. Ovarian torsion: Complete or partial torsion of ovary on its pedicle vascular supply due to long & flexible mesoovary. It accounts for approximately 3% of all cases of children with acute abdominal pain. More common in adolescents after menarche. The presence of vomiting, short duration of abdominal pain, and elevated CRP level (>5 mg/L) have a predictive value for the diagnosis of OT.
- 40. A 13 year old female, with acute ovarian torsion. The right ovary is in the mid-line, enlarged, measures 4.5 cm in largest diameter, with a volume of 33 ml, compared to left ovary which was 10 ml (not shown). Multiple peripheral small follicles seen. Lack of arterial and venous blood flow.
- 41. TUS in Detection of Small Bowel Tumors The most frequently visualized tumors of SB are localized in duodenum and terminal ileum. Tumors in other parts of SB can be viewed after gaining significant volume and are causing clinical symptomatology. Among the malignant tumors are more frequent adenocarcinoma localized prevalently in duodenum, then Carcinoid with prevalent localization in terminal ileum, followed by lymphomas in ileum and jejunum, and less frequent mesenchymal tumors, predominantly in jejunum. Most of the adenocarcinoma occurred in the duodenum and their relative frequency decreased in aboral direction: 29.9% in the jejunum and 16.0% in the ileum. The carcinoids showed an opposite trend, an increasing relative frequency in aboral direction: 3.9% in the duodenum, 9.2% in the jejunum and 86.7% in the ileum. Lymphomas were more frequent in the ileum (49.5%) compared to jejunum (29.4%) and duodenum (21.0%). Most sarcomas occurred along the jejunum (46.7%). Carcinoid tumors are oval hypoechogenic vascularised lesions and , lymphomas circularly affecting bowel segment with stenosis and dilatations of lumen. Most of gastro-intestinal lymphomas cause circumferential involvement of the bowel wall. Metastatic tumors of SB as well as benign tumors are sporadically visualized by TUS due to intussusception caused by these tumors.
- 42. Tumors of small bowel. (a) Solid oval tumor in the lumen of terminal ileum with hypervascularization in CFD (a) High resolution probe. (b) Oval solid tumor in D2 segment of duodenum—Standard abdominal probe. (e) Longitudinal section of thickened small bowel loop (S) with stenosis and dilatation (D) of lumen. Standard abdominal probe. (f)Transversal view with high resolution probe in dilated segment shows hypervascularization of thickened wall (f). Surgery confirmed suspected T-lymphoma of jejunum in untreated celiac disease.
- 43. Conventional ultrasound (US) is the recommended imaging method for lymph node (LN) diseases with the advantages of high resolution, real time evaluation and relative low costs. Current indications of transcutaneous ultrasound and endoscopic ultrasound include the detection and characterization of lymph nodes and the guidance for LN biopsy. Recent advances in US technology, such as contrast enhanced ultrasound (CEUS), contrast enhanced endoscopic ultrasound (CE-EUS), and real time elastography show potential to improve the accuracy of US for the differential diagnosis of benign and malignant lymph nodes. In addition, CEUS and CE-EUS have been also used for the guidance of fine needle aspiration and assessment of treatment response. Complementary to size criteria, CEUS could also be used to evaluate response of tumor angiogenesis to antiangiogenic therapies. In this paper we review current literature regarding evaluation of lymphadenopathy by new and innovative US techniques. Lymph node.
- 44. Homogeneous hyperenhancement(Lymphoma). Left figure: the CEUS mode, the red circle: lymph node; Right figure: the comparative gray-scale ultrasonography.
- 45. Inhomogeneous hyperenhancement(Metastasis). Left figure: the CEUS mode, the red circle: lymph node; Right figure: the comparative gray-scale ultrasonography.
- 46. Circle enhancement (Tuberculosis). Left figure: the CEUS mode, the red circle: lymph node, the yellow circle: surrounding tissue, the blue circle: artery; Right figure: the comparative gray-scale ultrasonography.
- 47. Isoenhancement (Reactive lymphadenopathy). Left figure: the CEUS mode, the red circle: lymph node; Right figure: the comparative gray-scale ultrasonography.
- 48. Non-Hodgkin’s lymphoma involving the inguinal region. A: Sonoelastography reliability test evaluation reveals typically asymmetric and circumscribed infiltrated harder (blue) lymph node tissue in low grade follicular cell lymphoma; B: Elastography (acoustic structured quantification) reveals mainly homogenous diffuse infiltration in high grade follicular cell lymphoma.
- 49. Colorectal carcinoma with presacral circumscribed lymph node metastasis proven by colonic endoscopic ultrasound using Fine Needle Aspiration Cytology. Sonoelastography reliability test evaluation reveals typically harder (blue) area in the lymph node.
- 50. Thank You.