Presentation1 radiological imaging of carpal tunnel syndrome.
•Download as PPTX, PDF•
17 likes•4,662 views

Health &medicine.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Presentation1 radiological imaging of carpal tunnel syndrome.
Similar to Presentation1 radiological imaging of carpal tunnel syndrome. (20)
More from Abdellah Nazeer
More from Abdellah Nazeer (20)
Recently uploaded
Recently uploaded (20)
Presentation1 radiological imaging of carpal tunnel syndrome.
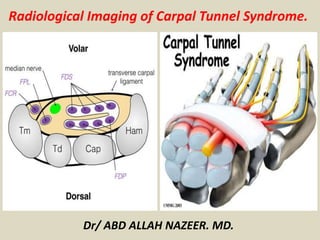
- 1. Radiological Imaging of Carpal Tunnel Syndrome. Dr/ ABD ALLAH NAZEER. MD.
- 2. Carpal tunnel syndrome (CTS) results from compression of the median nerve within the carpal tunnel. It is a cause of significant disability, and is one of three common median nerve entrapment syndromes; the other two being anterior interosseous nerve syndrome and pronator teres syndrome. Epidemiology Prevalence of CTS is estimated to be 2-4% of the adult ultrasound population, translating to 4-10 million patients, with a lifetime incidence of 10-15%, dependent upon occupational risk . Carpal tunnel syndrome usually occurs between the ages of 36 and 60 years and is two to five times more common in women than in men.
- 3. Clinical presentation CTS is primarily defined by pain and sensory symptoms: a typical symptom is brachialgia paresthetica nocturna, or nocturnal ascending pain emanating from the wrist sensory symptoms affect the first three digits and, depending on innervation patterns, the radial aspect of the fourth digit positive Tinel test (parasthesia elicited by tapping the median at the wrist) and Phalen test (parasthesia caused by wrist flexion over 30-60 s) are typical, as well hand weakness, as a rule, is a late and often functionally non-relevant symptom The dominant hand is affected more frequently, and bilateral involvement has been reported to occur in ~30% (range 8-50%) of cases. Clinical presentation can harbor some pitfalls. Sensory and pain symptoms of the pronator teres syndrome (PTS) and CTS can overlap - one can distinguish the two by examining for numbness of the forearm, which does not occur in CTS, and asking about nocturnal exacerbation, which would be atypical in PTS. Provocation tests as detailed above can help further.
- 4. Pathology There is a wide spectrum of causative pathologies, converging on two mechanisms of disease. Osteoarthritis, trauma, acromegaly, and mechanical overuse, among others, cause the carpal tunnel to decrease in size, whereas other disease states lead to augmentation of the contents of the carpal tunnel, both leading to entrapment: masses (e.g. ganglion cysts, primary nerve sheath tumors), deposition of foreign material (e.g. amyloid), or synovial hypertrophy in rheumatoid arthritis, to name a few. Radiographic features Ultrasound and MRI are the two imaging modalities which best lend themselves to investigating entrapment syndromes. Next to directly visualizing direct causes [e.g. primary nerve or sheath tumors, ganglion cysts, osseous spurs, anatomical variants (e.g. Gantzer muscle), recognizing pathological muscle signal patterns on MRI can inversely point to the affected nerve.
- 5. Ultrasound In imaging median nerve syndromes, ultrasound is useful in examining CTS, potentially revealing, in fully developed cases, a triad of: palmer bowing of the flexor retinaculum (>2 mm beyond a line connecting the pisiform and the scaphoid) distal flattening of the nerve enlargement of the nerve proximal to the flexor retinaculum Enlargement of the nerve seems to be the most sensitive and specific criterion, but what cut-off value for pathological size remains debated; normal cross-sectional area is given at 9-11 mm ², but the range of sizes deemed pathological is wide. One study has calculated that a 2 mm ² difference in nerve cross- section between the level of the pronator quadratus and the carpal tunnel has a 99% sensitivity and 100% specificity for CTS. Some of the other proposed findings include a flattening ratio of over 3 bowing of the retinaculum > 4 mm
- 6. MRI In CTS, MRI can demonstrate palmer bowing of the flexor retinaculum, enlargement of the median nerve at the level of the pisiform, and flattening of the median nerve at the level of the hook of the hamate. Other signs are edema or loss of fat within the carpal tunnel, and increased size/edema of the nerve on water-sensitive sequences, and, in some cases, contrast enhancement of the nerve. Although sensitivity and specificity of MRI in CTS are low (23-96% and 39-87%, respectively), MRI is especially well-suited for detecting masses, arthritic changes, or normal variants.
- 7. Carpal tunnel syndrome (A) and CT scan (B) shows that calcifying mass is located just above the capitate.
- 8. Carpal tunnel syndrome. Transverse (a) and longitudinal (b) US scans of a patient with CTS, showing a hypoechoic median nerve without the normal fascicular pattern, with a CSA of 16 mm2 measured at the level of the proximal tunnel. CSA measurements should be obtained within (dotted line) rather than outside the echogenic epineurium (open arrows).
- 9. Median nerve CSA measurements of a patient with CTS. Transverse US scans of a patient with CTS, showing median nerve (arrows) CSA measurements at the distal forearm (a), between the flexor pollicis longus (FPL) and the flexor digitorum superficialis (FDS), and at the wrist (b), at the level of maximal nerve swelling. ΔCSA = 13 – 8,5; ΔCSA =4,5 mm2.
- 10. Bifid median nerve and persistent median artery. Transverse US scans of two patients with bifid median nerves (dotted lines), in b) accompanied by a persistent median artery (arrow).
- 11. Segmental enlargement of the median nerve ahead of the stenosis and flattening in the carpal tunnel (white arrows head) below the flexor retinaculum (small white arrows) corresponding to the notch sign. Increased intraneural blood flow within the enlarged nerve at color Doppler (small orange arrows).
- 12. Rheumatoid nodule. Transverse (a) and longitudinal (b) US scans of a patient with long-standing Rheumatoid Arthritis and unilateral CTS, in which a hypoechoic nodule (open arrows) was identified, adjacent to and dislocating the median nerve (dashed arrows). Additionally, this patient had two persistent median arteries.
- 13. Median nerve schwannoma. Longitudinal (a) and transverse US scans of a patient with unilateral CTS symptoms, showing an oval-shaped, homogenous hypoechoic tumor (open arrows) arising from the median nerve (dashed arrows).
- 14. Axial T1 et T2FS : T1: enlarged median nerve T2: nerve signal increase. The normal fascicular appearance of the nerve has disappeared
- 15. Sagittal T1FS after IV injection of contrast Median nerve neuroma enhancement after intravenous injection of gadolinium.
- 16. Segmental swelling of median nerve (arrows). Axial MR images (TR 2000, TE 20) at levels of pisiform (A) and hook of hamate (B). Left wrist viewed toward elbow with palm down. Note enlargement of nerve proximally (A) compared with normal caliber of nerve distally (B).
- 17. Diffuse swelling of median nerve (arrows). Axial MR images (TR 2000, TE 60) of left wrist viewed toward elbow with palm down in patient with bilateral postpartum carpal tunnel syndrome. Note enlargement as well as markedly increased signal intensity at both level of pisiform (A) and level of hook of hamate (B). Right wrist had similar appearance.
- 18. Carpal Tunnel Syndrome with swelling and bright signal within the median nerve .
- 19. Carpal Tunnel Syndrome with swelling and bright signal within the median nerve .
- 20. These images reflect an enlarged nerve containing prominent, irregular fascicles with increased T2 signal intensity. T1 and STIR T2 images of an abnormally flattened median nerve at its flattest point. MRI can reliably be used to quantitatively measure the median nerve in the carpal tunnel. Limitations include resolution at the edge of the coil, which may be responsible for poorer inter-reader reliability at the proximal metacarpal joint. Reliability was poorer for determining abnormally bright median nerve signal and the locations where the median nerve was 'flattest' and 'largest'.
- 21. Carpal Tunnel Syndrome. Axial FS post contrast MR at the wrist shows an enhancing median nerve (arrowed).
- 22. Magnetic resonance imaging of carpal tunnel showing T2-weighted hyperintensity of median nerve (arrow) and thenar and hypothenar muscles (asterisks)
- 23. (a) Wrist of a patient with severe CTS at the level of the distal part of the distal radioulnar joint. The median nerve is enlarged and can be seen as a high-intensity area on the MRI. Insertion from the entry point close to the ulnar side of the PL results in contact between the needle and the nerve. Insertion from C and D leaves a narrow margin between the needle and the nerve. *Median nerve. (b) Wrist of a patient with extremely severe CTS. At the level of the distal part of the distal radioulnar joint, the median nerve is enlarged and can be seen as a high-intensity area on the MRI. Insertion from the entry point close to the ulnar side of the PL and FCR results in contact between the needle and the nerve. *Median nerve.
- 25. Magnetic resonance imaging of carpal tunnel showing T2-weighted hyperintensity of median nerve (arrow)
- 26. (A) MRI shows hypertrophied palmaris longus is compressing median nerve in carpal tunnel (white arrow: hypertrophied palmaris longus muscle). (B) Open transverse carpal ligament release and hypertrophied palmaris longus excision was performed.
- 29. MRI of the lesion (L) shows it a) attached to the index finger profundus tendon in the coronal plane on T1 weighted imaging, b) demonstrating septal enhancement post contrast administration, c) displacing the superficialis tendons (T) to the middle and index fingers radially on axial T1 imaging, and d) showing heterogeneous T2 hyperintensity again in the axial plane, with the compressed median nerve (N) more clearly visualized.
- 30. Fibrolipomatous hamartoma of the median nerve presenting with carpal tunnel syndrome.
- 31. There is evidence of mixed signal intensity oblong lesion with fatty and low signal intensity areas in the carpal tunnel with bulging of the flexor retinaculum. Differentials include perineural lipomatous lesion of the median nerve.
- 32. Sarcoidosis of the carpal tunnel with Carpal Tunnel Syndrome.
- 33. Lipoma of the carpal tunnel with Carpal Tunnel Syndrome.
- 35. Thank You.