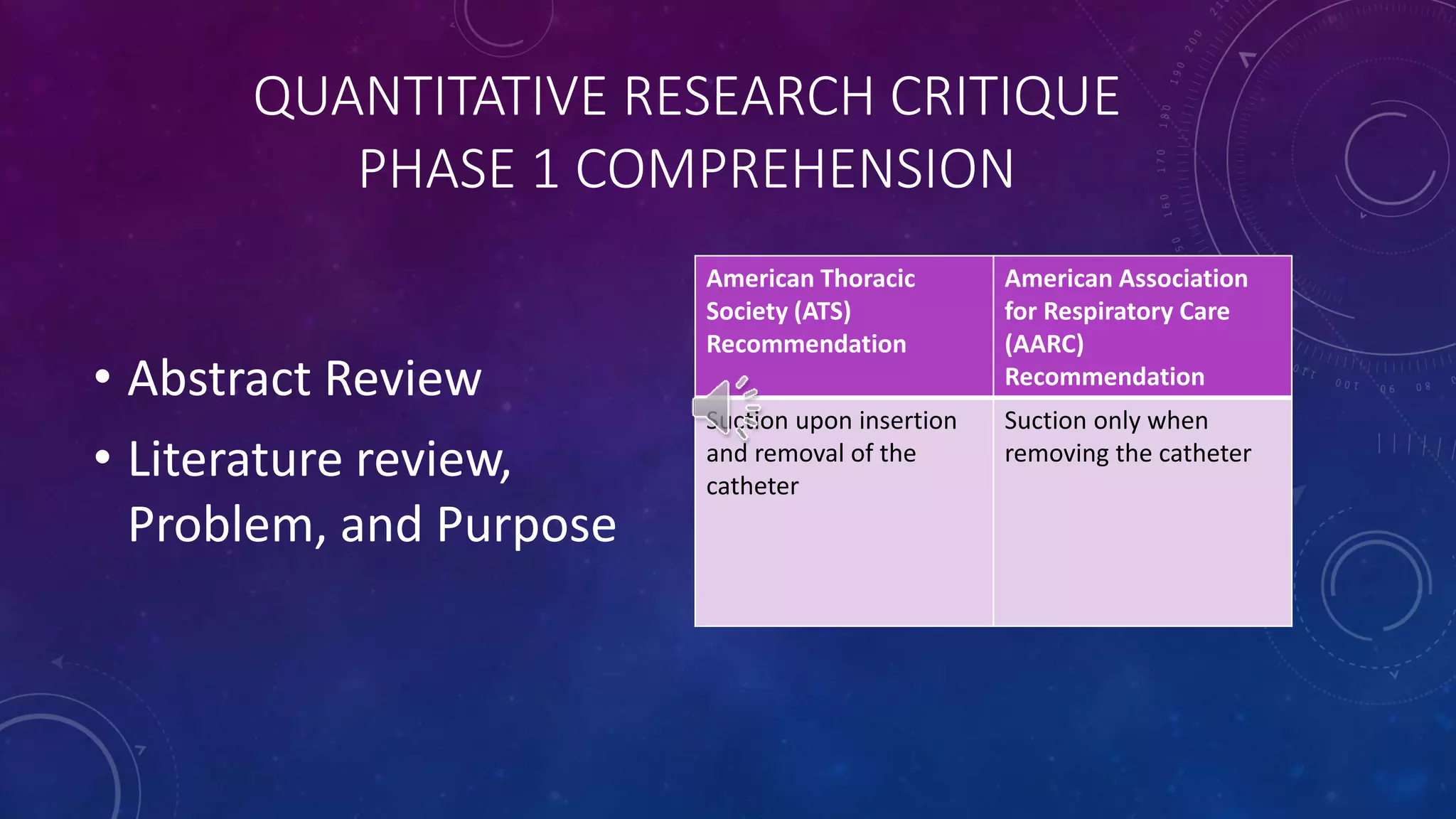
This document outlines the phases of a quantitative research critique being conducted by Jessica Clark on a pilot study comparing two methods of tracheal suctioning in children with chronic tracheostomies. The critique will include 4 phases: comprehension of the study, comparison and analysis of the research problem/purpose, literature review, and design, evaluation of bias, measurements, sample/setting, data collection and interpretation of findings. The document provides details on the independent and dependent variables, procedures, and limitations of the pilot study being critiqued.