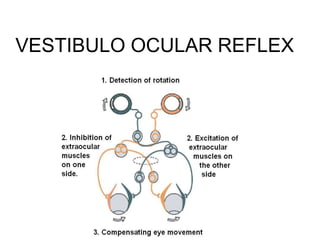
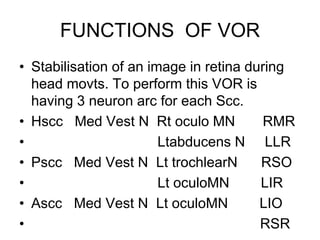
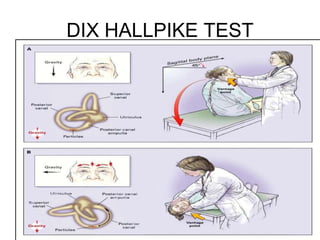
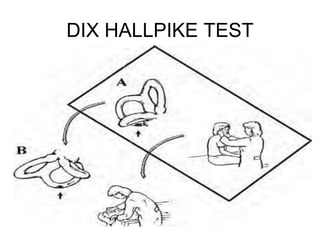
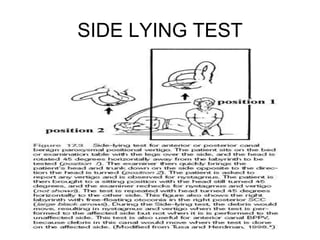
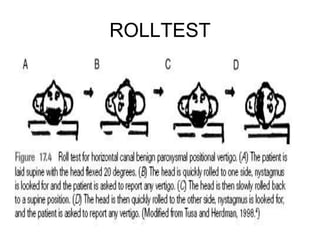
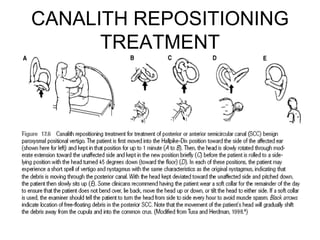
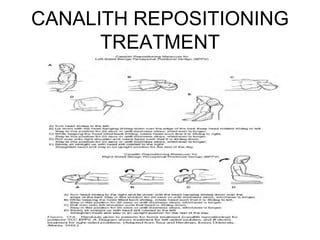
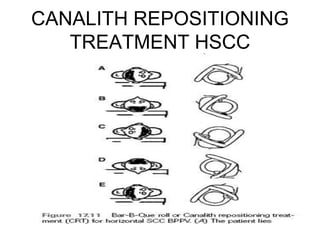
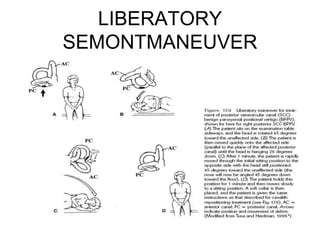
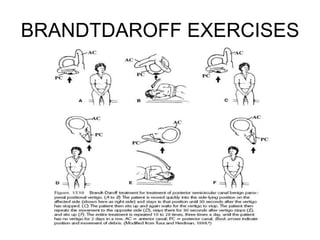
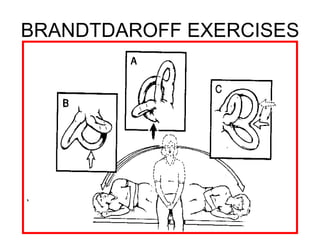
This document provides an overview of vestibular and balance rehabilitation. It discusses the anatomy and physiology of the vestibular system, common vestibular system dysfunctions, evaluation techniques, and physical therapy management strategies. Evaluation techniques include tests like Dix-Hallpike, side lying, and roll tests to assess nystagmus. Physical therapy management uses exercises like canalith repositioning, Epley maneuver, Brandt-Daroff exercises, and habituation exercises to treat conditions like BPPV and vestibular hypofunction.




























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)








