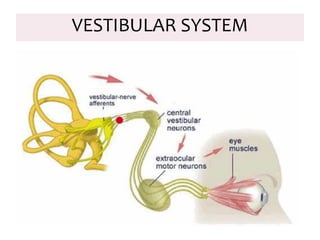
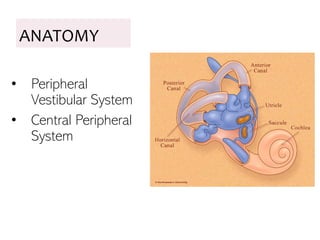
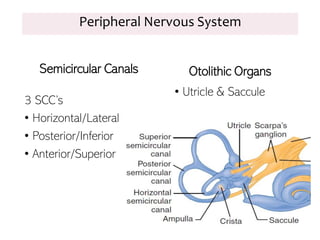
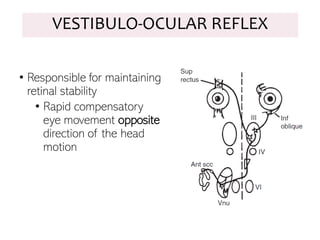
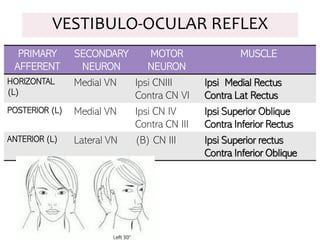
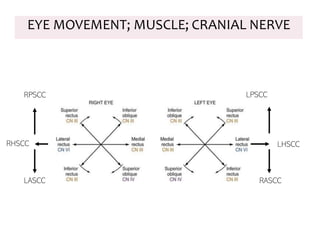
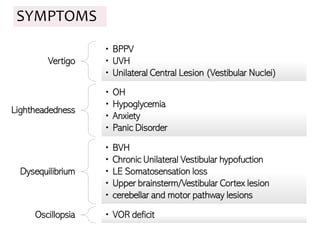
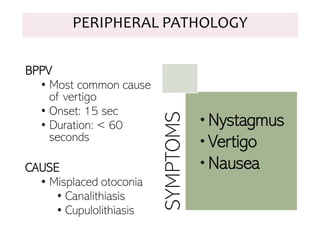
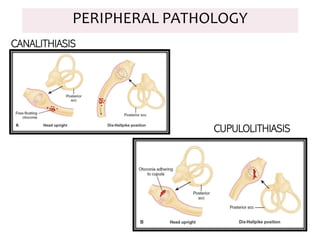
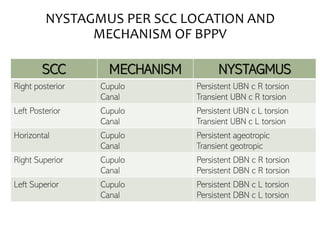
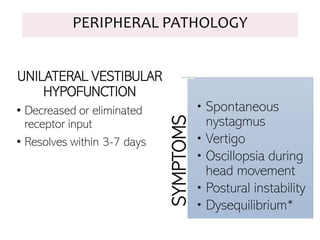
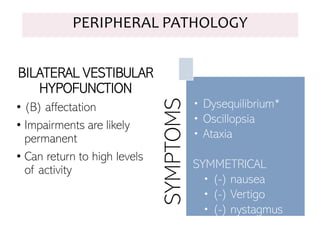
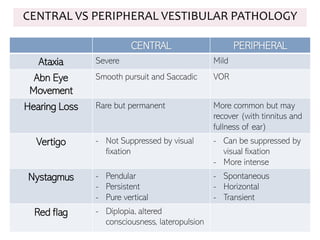
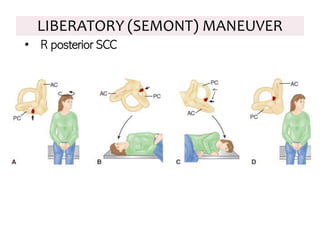
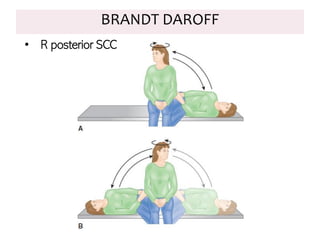
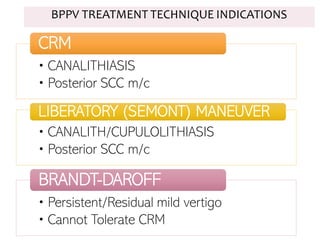
The document details the anatomy and functions of the vestibular system, including its components like the semicircular canals and otolithic organs, and describes various vestibular disorders such as BPPV and unilateral vestibular hypofunction. It covers assessment techniques for vestibular function and treatment strategies for disorders, including canalith repositioning maneuvers and balance exercises. Additionally, the document emphasizes the differences between central and peripheral vestibular pathologies in terms of symptoms and recovery outcomes.