Downloaded 602 times

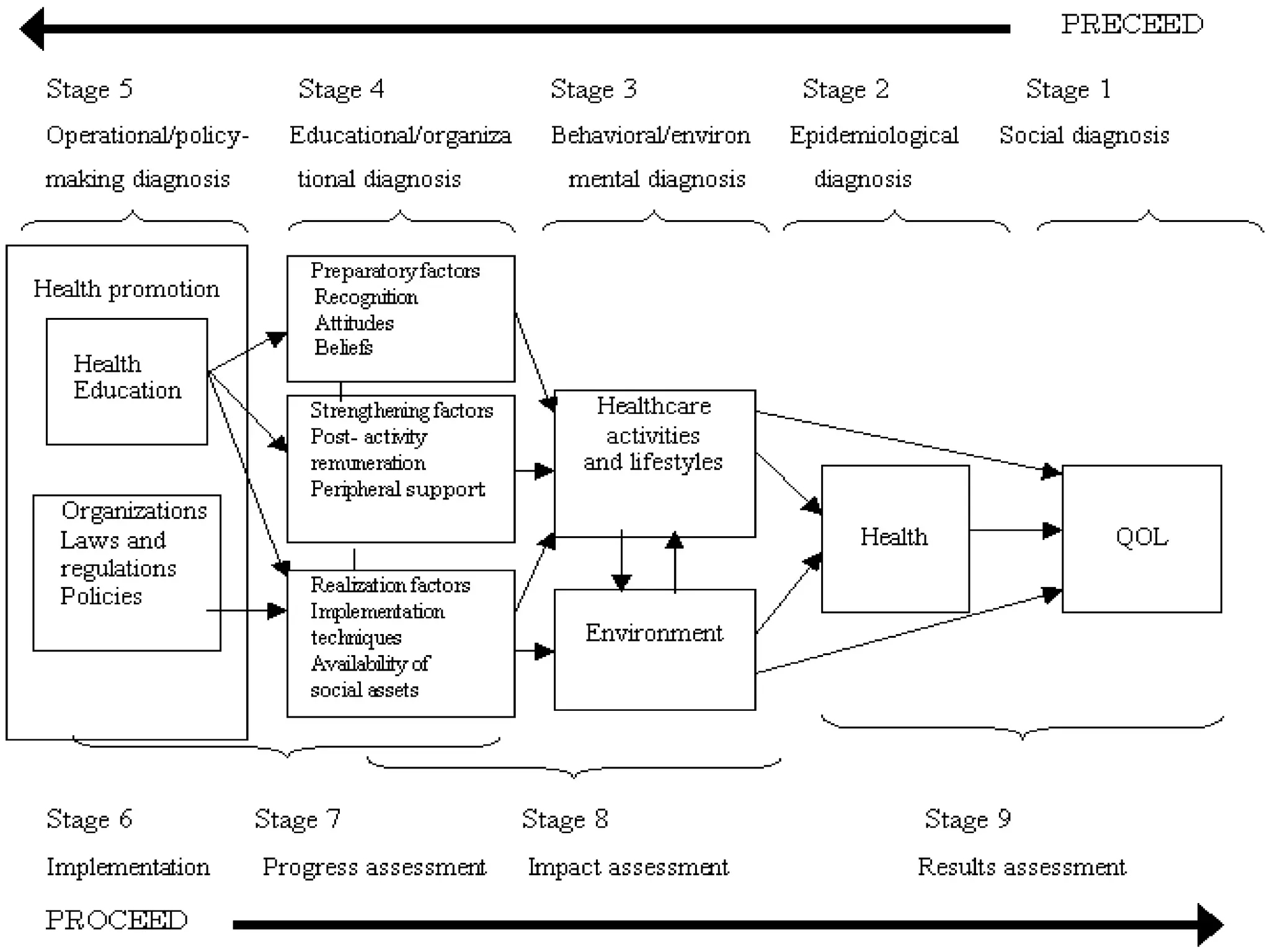

The PRECEDE-PROCEED model provides a comprehensive framework for designing, implementing, and evaluating health promotion programs. It consists of 9 phases: (1) social diagnosis to identify community health issues, (2) epidemiological diagnosis to determine associated health problems, (3) behavioral and environmental diagnosis to analyze behavioral and environmental factors, (4) educational diagnosis to select factors to modify behaviors, (5) administrative diagnosis to assess resources and policies, (6) implementation, (7) process evaluation, (8) impact evaluation, and (9) outcome evaluation to determine effects on health and quality of life. The model takes a participatory approach and considers both individual and environmental influences on behaviors.






























































































