






















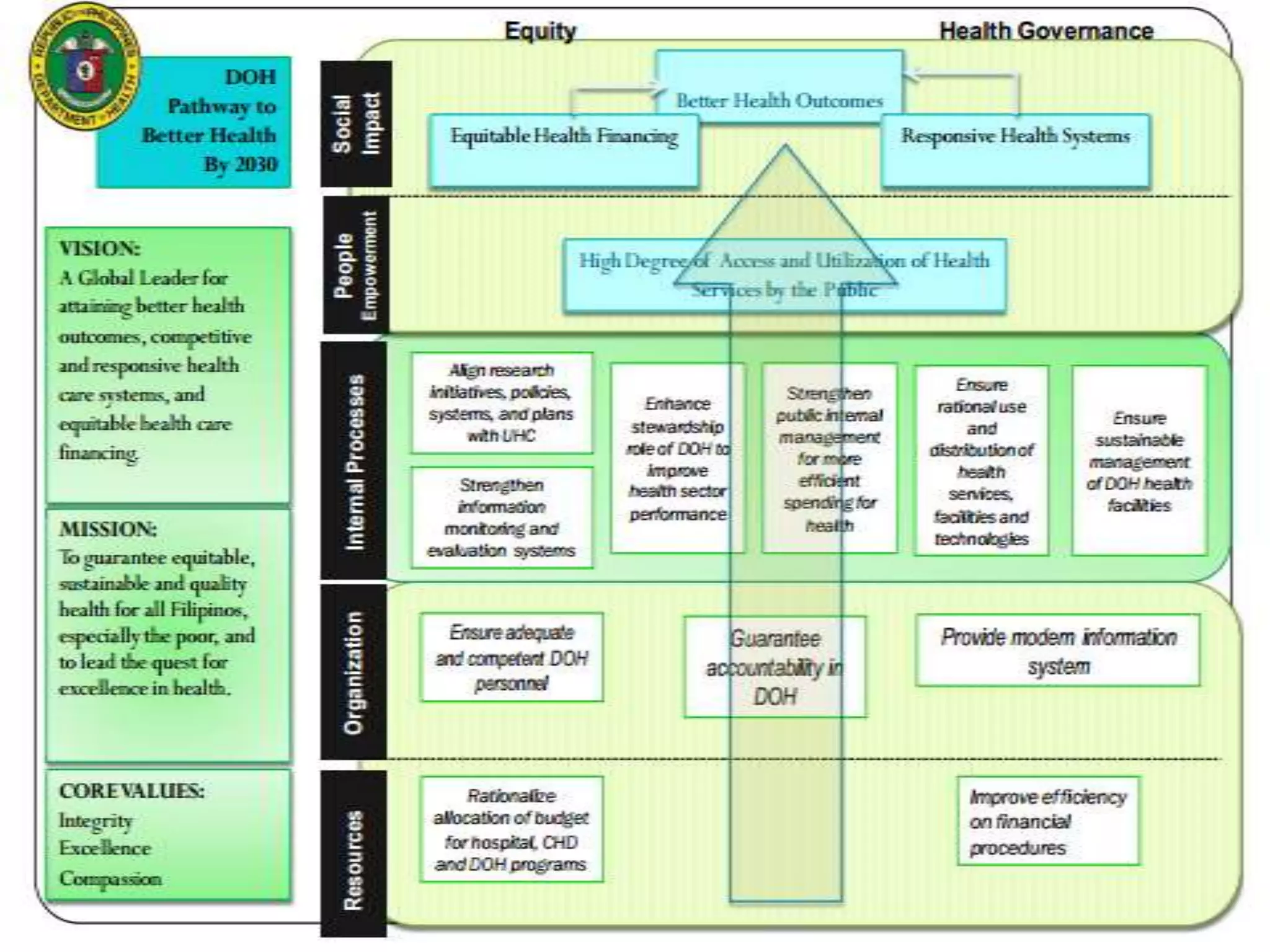











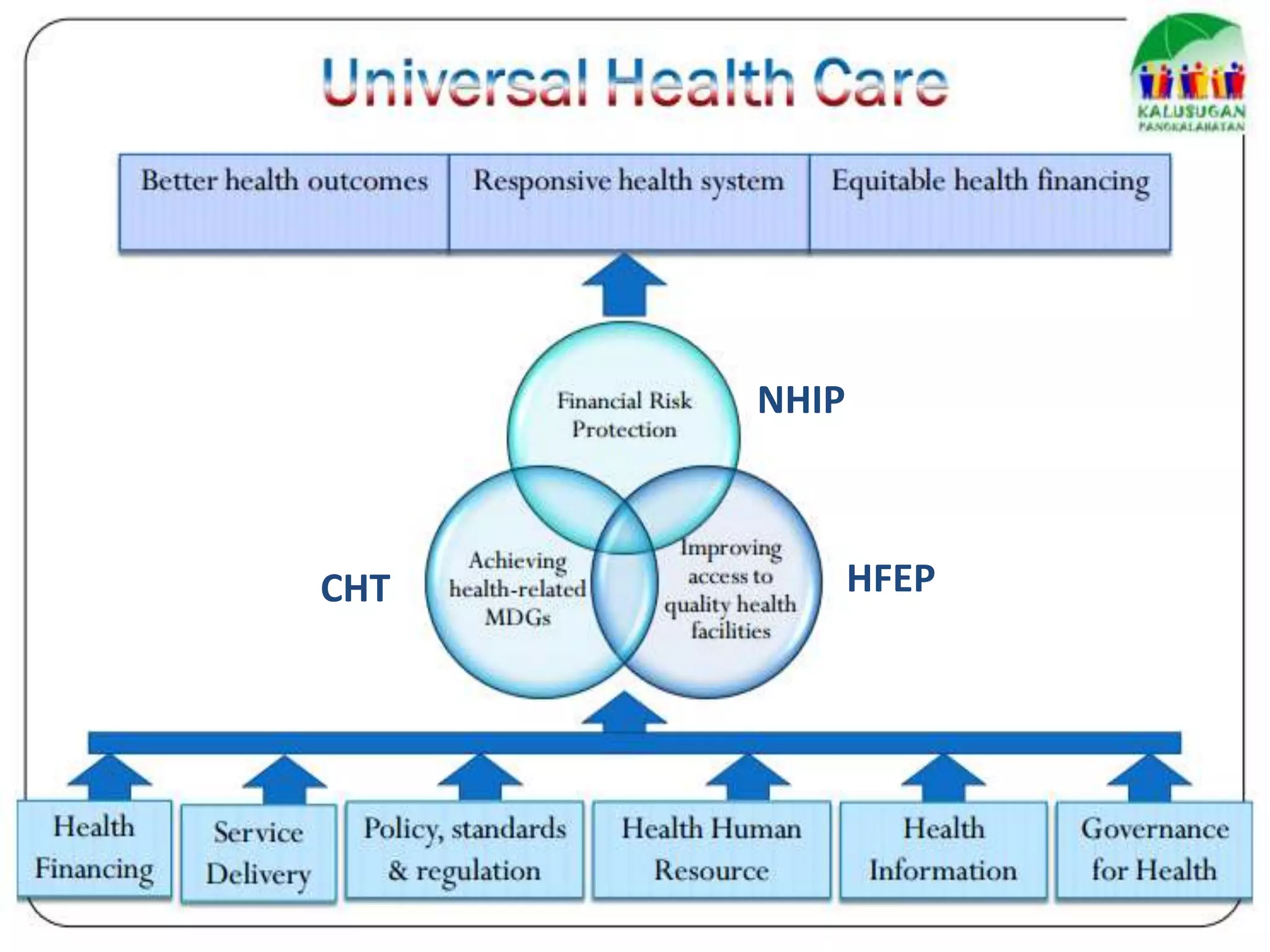




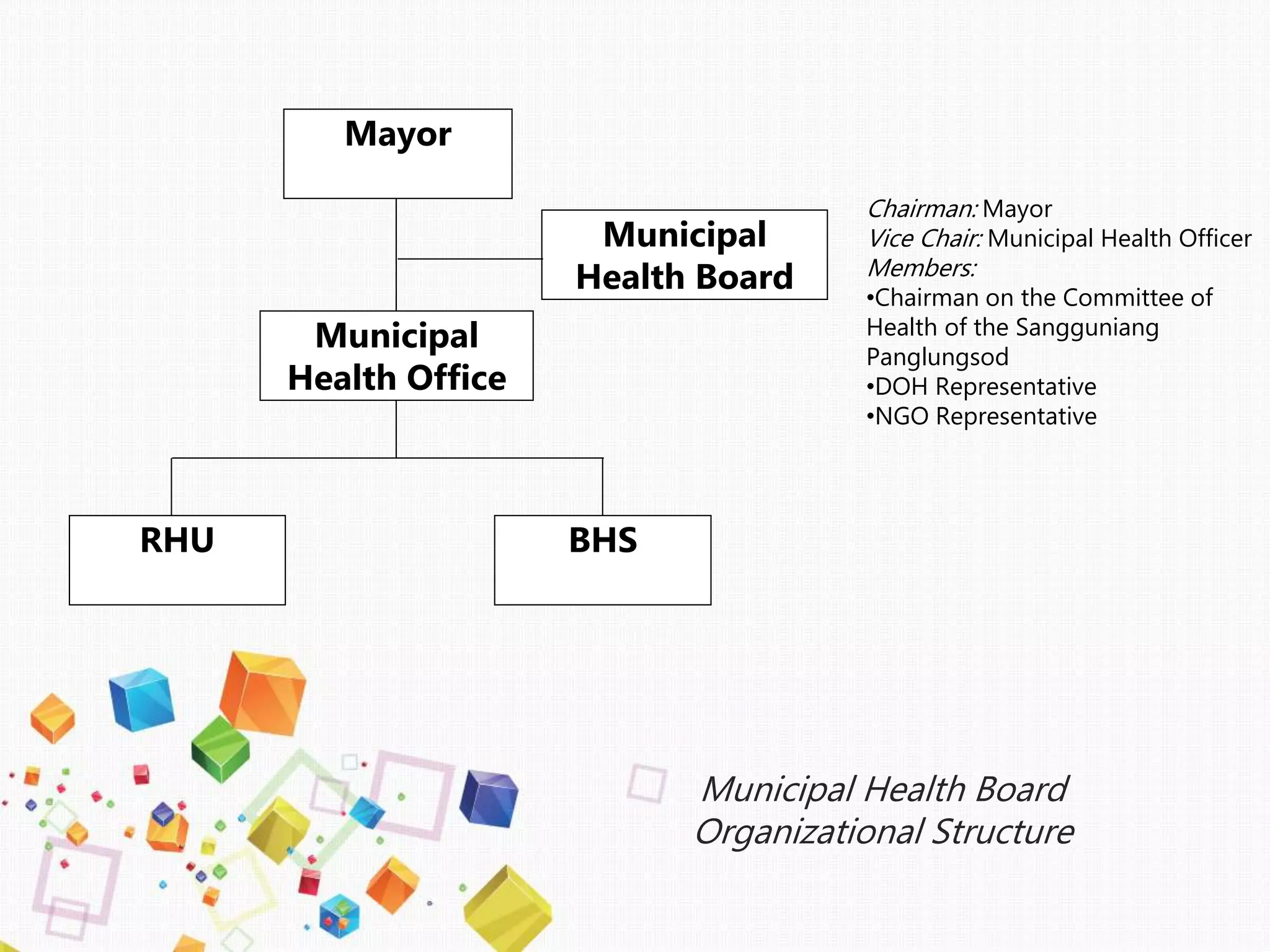



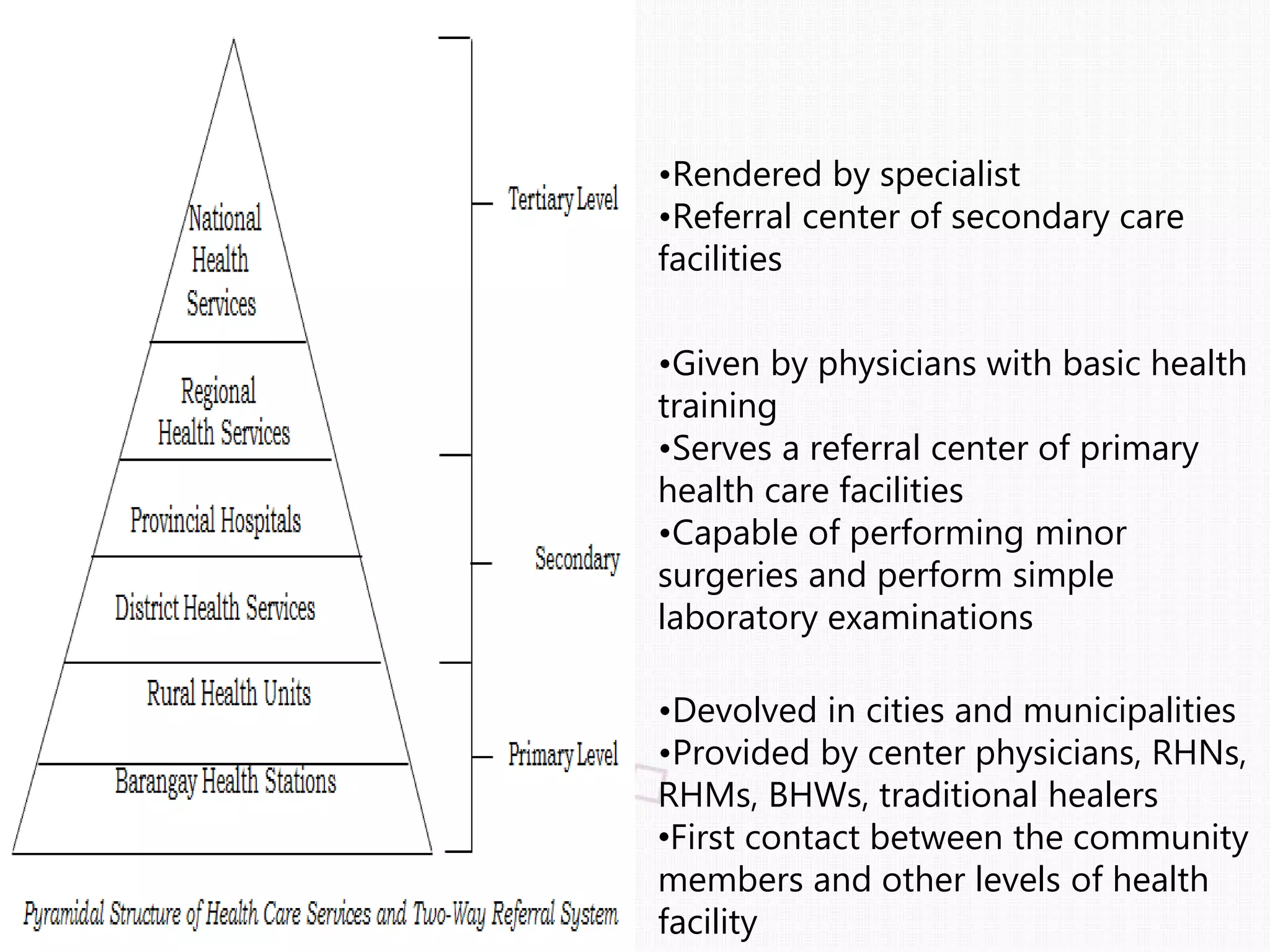












The document outlines the Philippine health care delivery system, defining health systems and their functions, and discussing challenges like high costs and workforce issues. It elaborates on the roles of the Department of Health, governance structures, and various health care models, including financing strategies and health reforms aimed at improving access and quality. Additionally, it emphasizes the need for a multisectoral approach and the implementation of universal health care to ensure equitable access for all Filipinos.











































































































