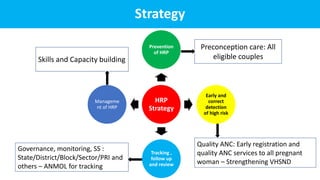
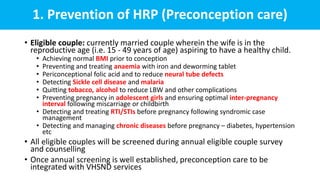
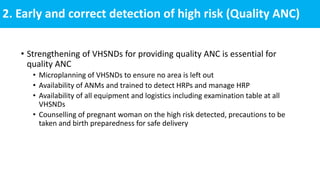
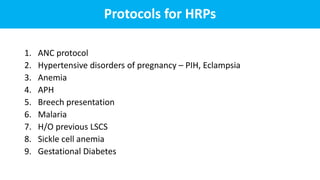
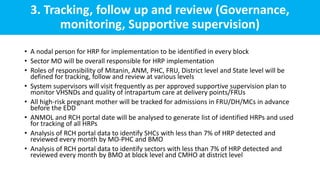
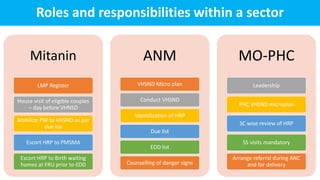
The document outlines strategies for the prevention, detection, tracking, and management of high-risk pregnancies (HRP) as part of maternal health services. It emphasizes the importance of quality antenatal care, early detection of HRP, and functional referral linkages between health facilities. Additionally, it details the roles and responsibilities of health care workers in providing preconception care, monitoring, and emergency response frameworks to enhance maternal and neonatal outcomes.