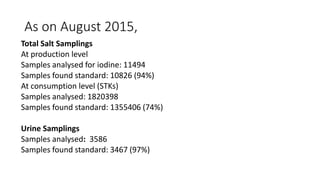
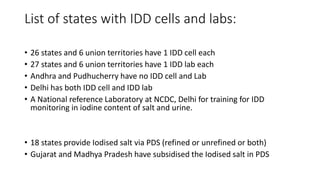
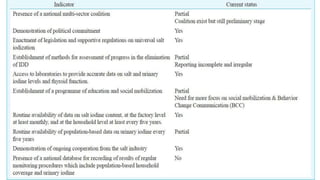
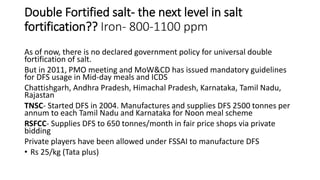
This document provides an overview of national iodine deficiency disorders control program in India. It discusses that iodine is essential for thyroid hormone production. Over 350 million Indians are at risk of iodine deficiency disorders. The program aims to reduce prevalence below 10% through universal salt iodization, surveys to assess magnitude, and health education. Key activities include iodizing salt, monitoring salt and urine iodine levels, and information campaigns. The program has helped control goiter and improved iodine nutrition, though some areas still face deficiencies.