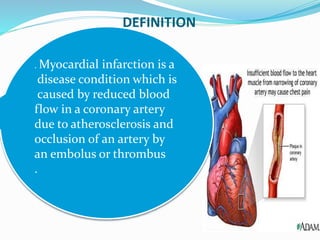
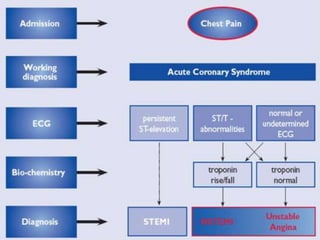
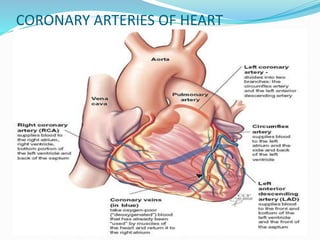
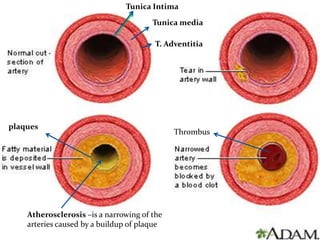
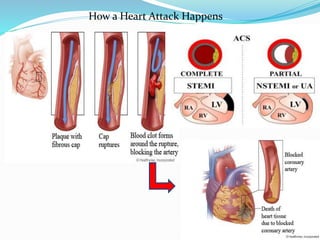
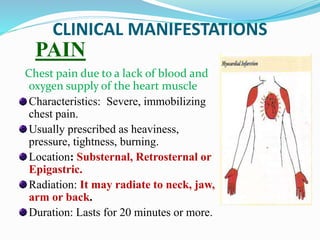
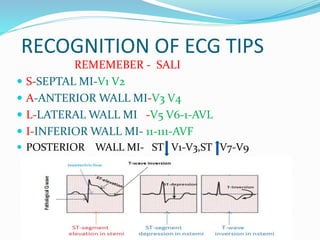
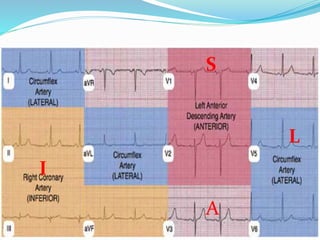
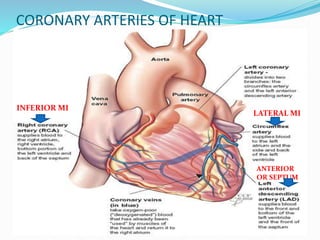
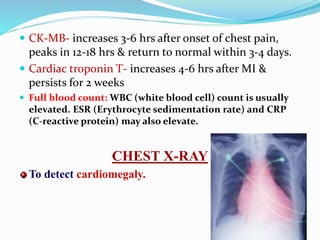
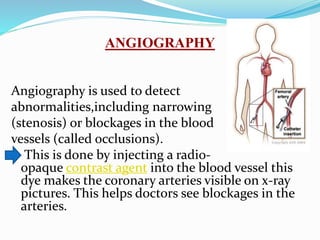
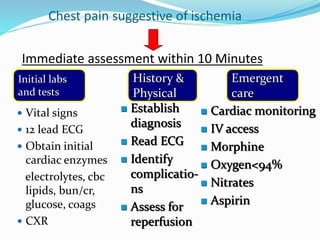
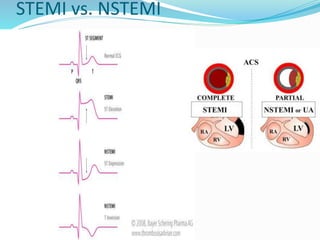
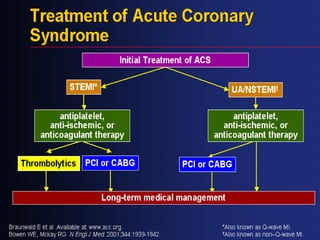
This document provides information about myocardial infarction (MI) or heart attack. It defines MI as reduced blood flow in a coronary artery due to atherosclerosis or blockage. MI is a leading cause of death. Risk factors include age, family history, smoking, hypertension, high cholesterol, diabetes and stress. Signs and symptoms include chest pain and shortness of breath. Diagnosis involves ECG, cardiac enzymes and angiography. Treatment includes aspirin, nitrates, beta blockers, statins, clot-busting drugs, angioplasty and bypass surgery. Complications can include arrhythmias, heart failure and heart rupture.