Downloaded 452 times

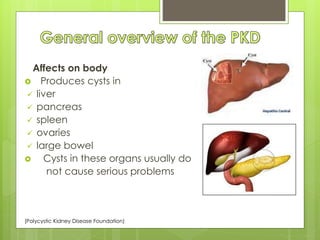
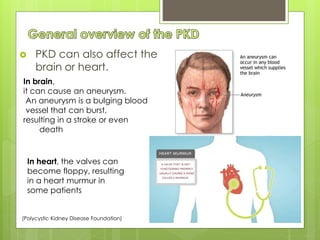
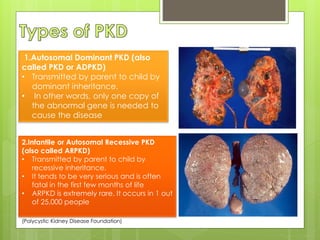
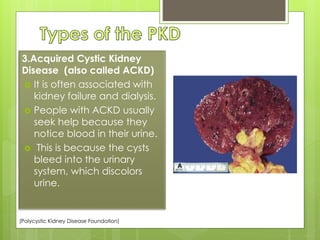
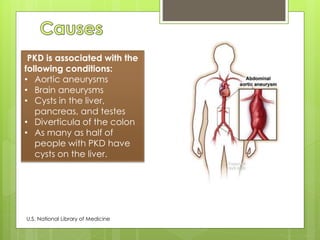
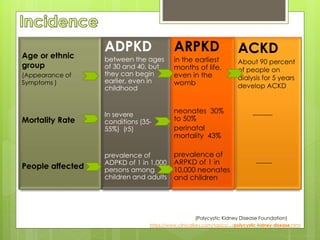


Polycystic Kidney Disease (PKD) is a hereditary condition characterized by the formation of cysts in various organs, most notably the kidneys, which can lead to serious complications such as high blood pressure and aneurysms. There are three main types of PKD: autosomal dominant PKD (ADPKD), which is common and manifests typically in adulthood, autosomal recessive PKD (ARPKD), which is rare and often fatal in infancy, and acquired cystic kidney disease (ACKD), associated with kidney failure. Currently, there is no cure for PKD, but management focuses on controlling symptoms and preventing complications.


































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)













