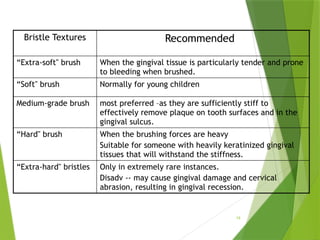
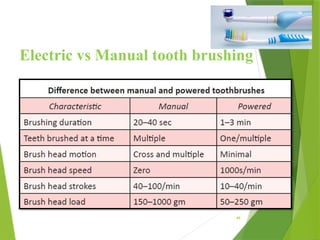
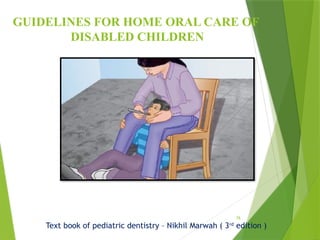
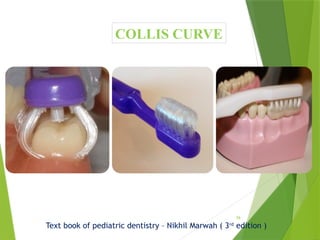
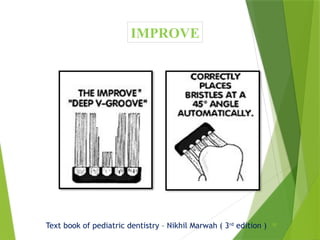
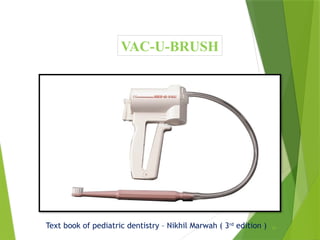
The document discusses methods of plaque control, focusing on both mechanical and chemical approaches. It details various types of toothbrushes, techniques for effective brushing, and the efficacy of dental floss in children, particularly contrasting traditional flossing with gumchucks. Additionally, it examines the properties and classifications of chemical plaque control agents, highlighting their role in oral hygiene.































































![PLAQUE CONTROL.ppt [Recovered].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/plaquecontrol-220827085644-ef330fe9-thumbnail.jpg?width=640&height=640&fit=bounds)





































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)